شرح المدرسين

Introduction
A multiple pregnancy occurs when two or more fetuses develop simultaneously in the womb. Distinguished into monozygotic (identical) and dizygotic (fraternal) categories, the management and outcomes of these pregnancies hinge on their classification. Monozygotic twins arise from a single fertilized oocyte dividing into two, while dizygotic twins result from the fertilization of two separate oocytes.
Epidemiology
The frequency of multiple births :
- Twins: ∼ 1:89¹
- Triplets: ∼ 1:89² (1:7,921)
- Quadruplets: ∼ 1:89³ (1:704,969)
Etiology
Factors increasing the likelihood of multiple pregnancies include :
- Advanced maternal age (≥ 35 years)
- Previous multiple pregnancy
- Use of assisted reproductive technology
- Maternal family history of dizygotic twins
Classification
- Monozygotic vs. Dizygotic Twins: Monozygotic twins share identical genetic material, while dizygotic twins are genetically distinct. The division of the amniotic sac and placenta varies, influencing the pregnancy's management and potential complications.
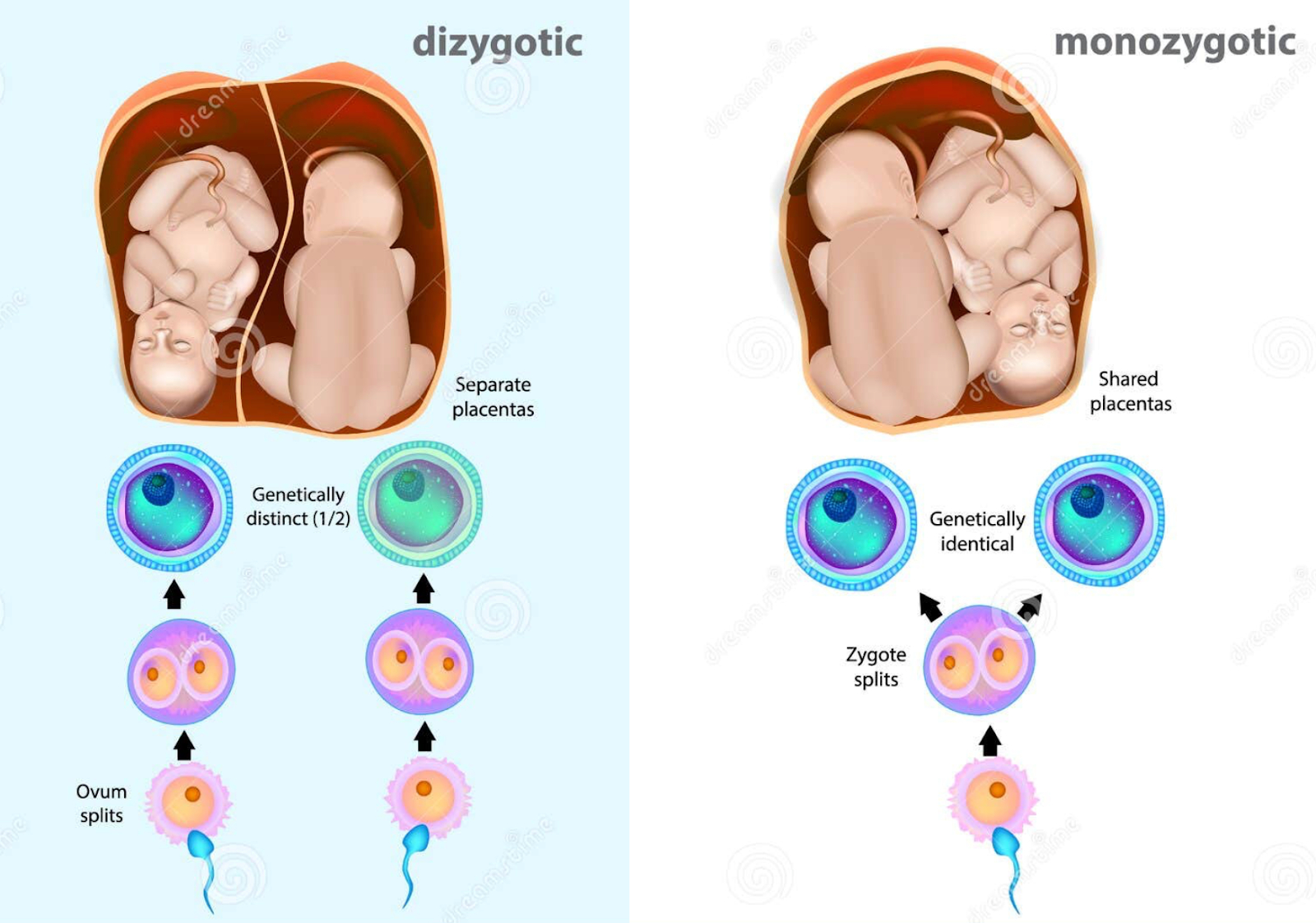
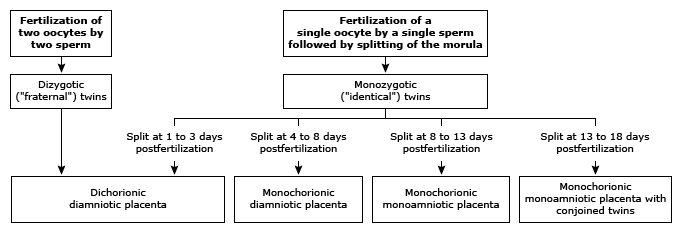
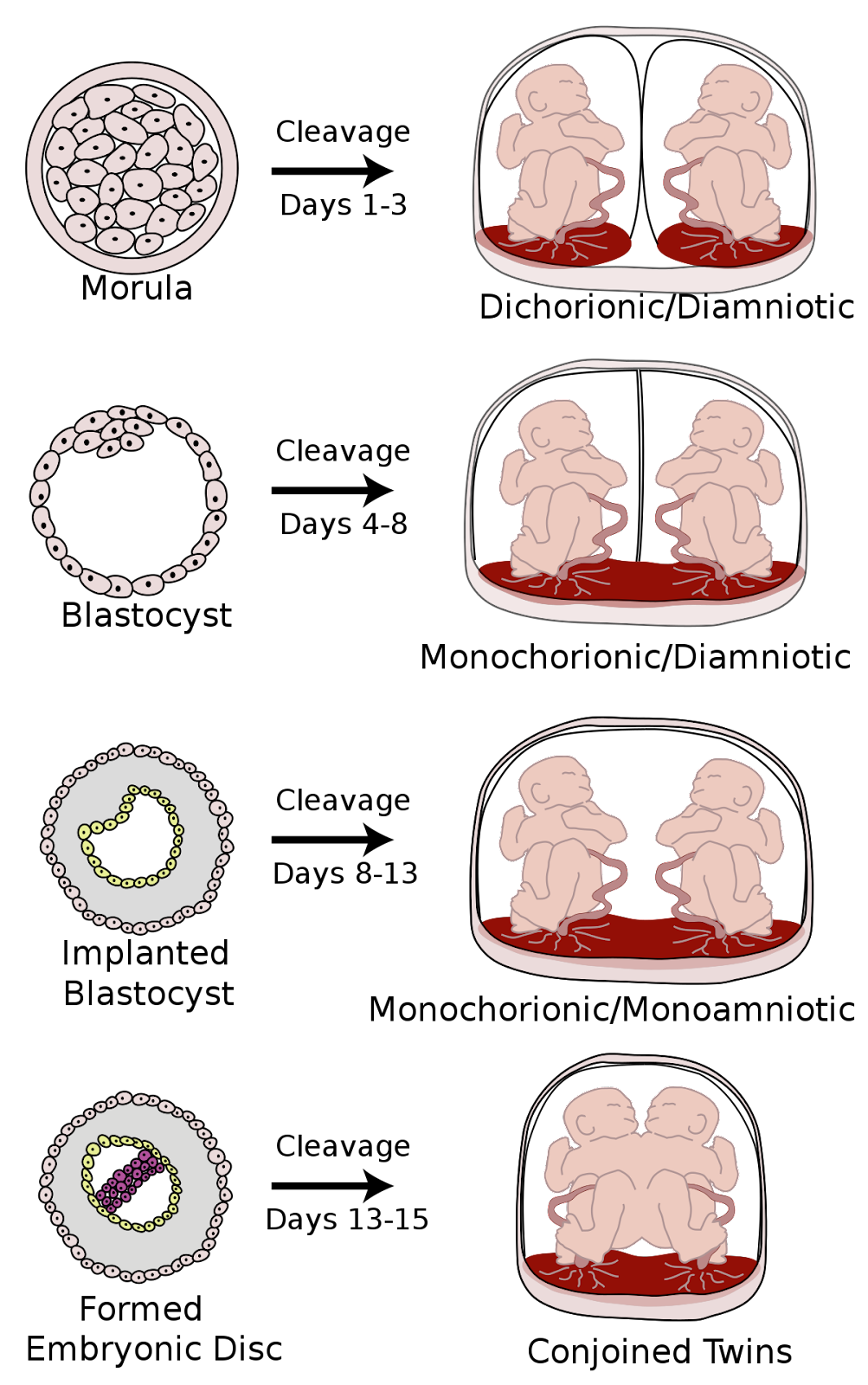
Comparison of monozygotic vs. dizygotic twins Identical twins (monozygotic twins) Fraternal twins (dizygotic twins) Frequency ⅓ of all twin pregnancies ⅔ of all twin pregnancies Origin Division of the fertilized oocyte into two embryonic layers Fertilization of two oocytes with two mature spermatozoa Genetics of the individual Genetically identical Genetically different Chorionic cavity and amniotic sac Varies Dichorionic-diamniotic - Development Variations in Monozygotic Twins: The timing of the zygotic division significantly affects chorionicity and amnionicity, ranging from dichorionic-diamniotic to monochorionic-monoamniotic, with the latter including the rare occurrence of conjoined twins.
Diagnosis
- Physical Examination: Notable findings include larger fundal height and abdominal girth for gestational age and detection of multiple fetal heart rates.
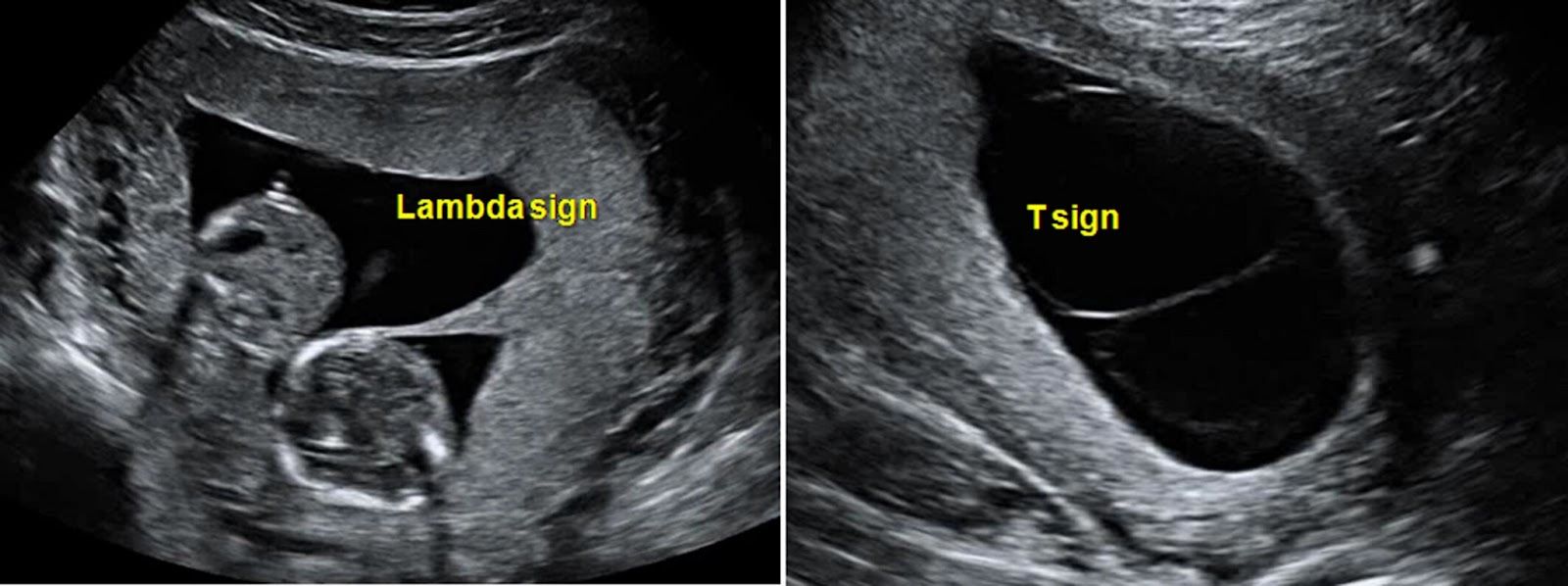
- Ultrasound: Essential for identifying multiple fetuses and determining chorionicity and amnionicity, with specific signs indicating dichorionic or monochorionic twins.
- Differentiating Twin Types Early On :
- Dichorionic Twins:
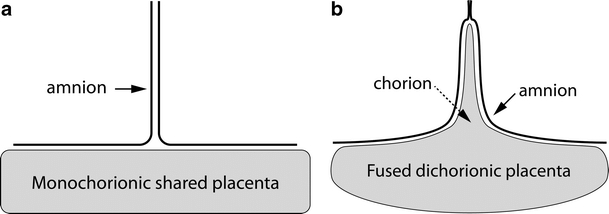
- Lambda Sign: Indicates twins with separate chorionic and amniotic sacs, seen as a λ-shaped separation on ultrasound.
- Monochorionic Twins:
- T-Sign: Suggests twins share a chorionic sac but have individual amniotic sacs, appearing as a T-shaped separation on ultrasound
- Dichorionic Twins:
- Differentiating Twin Types Early On :
Complications
Multiple pregnancies heighten the risk of numerous complications:
- Maternal:
- Preterm Labor and Birth: The most common complication, leading to early delivery.
- Hyperemesis Gravidarum: Severe nausea and vomiting.
- Gestational Diabetes: High blood sugar that develops during pregnancy.
- Preeclampsia/Eclampsia: High blood pressure leading to seizures in severe cases.
- Pregnancy-Induced Hypertension: High blood pressure due to pregnancy.
- Cervical Incompetence: Premature dilation of the cervix, leading to potential preterm birth.
- Premature Rupture of Membranes: Early breaking of waters before labor begins.
- Placental Insufficiency and Hypotrophy: Reduced function of the placenta, affecting fetal nutrition and growth.
- Intrauterine Malnutrition: At least one fetus does not receive adequate nutrition.
- Uterine Atony: Lack of muscle tone in the uterus after birth, leading to heavy bleeding.
- Miscarriage or Loss of One Fetus: During the first trimester, sometimes known as vanishing twin syndrome.
- Placenta Previa: Placenta covers the cervix, causing bleeding during pregnancy.
- Birth Complications: Including prolonged labor, placental abruption (placenta detaches prematurely), and prolapsed cord (umbilical cord drops through the cervix).
- Fetal:
- Spontaneous Reduction or Vanishing Twin Syndrome: A phenomenon where one of the twins disappears from the ultrasound and is absorbed by the other twin or the mother's body during the first trimester.

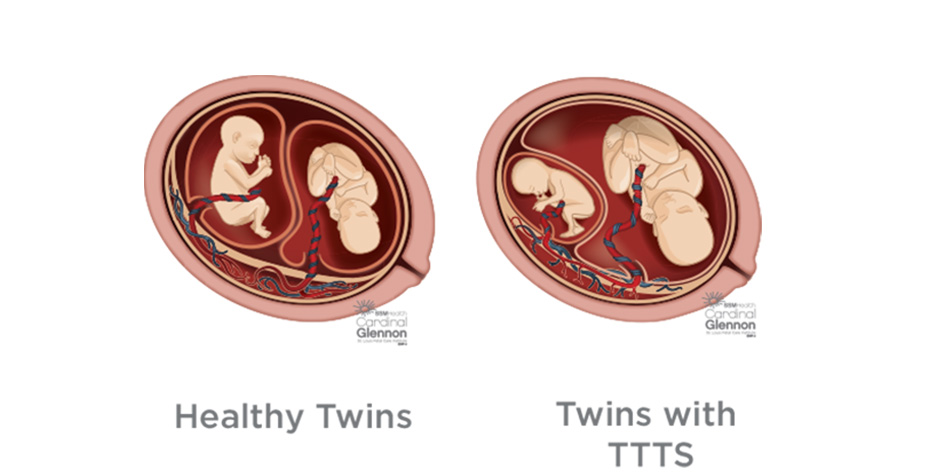
- Twin-to-Twin Transfusion Syndrome (TTTS): Affects 10-15% of monochorionic twin pregnancies (twins sharing the same placenta). This condition occurs when blood is unevenly exchanged between the twins through vascular connections on the shared placenta, leading to imbalances in blood volume.
- Recipient Twin Complications:
- Polycythemia: An abnormally high concentration of red blood cells.
- Hypervolemia: Increased blood volume.
- Polyhydramnios: Excessive amniotic fluid in diamniotic pregnancies, leading to increased risk of preterm labor.
- Donor Twin Complications:
- Anemia: Low levels of red blood cells.
- Growth Retardation: Slower than normal fetal growth.
- Hypovolemia and Dehydration: Reduced blood volume and fluid, sometimes leading to a "stuck twin" appearance where the twin is immobile due to oligohydramnios (reduced amniotic fluid).
- Oligohydramnios: Low levels of amniotic fluid in diamniotic pregnancies, increasing the risk of limb deformities, lung hypoplasia, and facial distortion.
- Cord Entanglement: This serious complication can only occur in monoamniotic twin pregnancies (twins sharing the same amniotic sac), leading to the risk of cord compression and compromised blood flow to one or both twins.
- Increased Risk of Neonatal Morbidity and Mortality: Multiple pregnancies are associated with higher risks of growth restrictions, prematurity, cerebral palsy, congenital abnormalities, and increased neonatal mortality rates.
- Recipient Twin Complications:
- Spontaneous Reduction or Vanishing Twin Syndrome: A phenomenon where one of the twins disappears from the ultrasound and is absorbed by the other twin or the mother's body during the first trimester.
Management
Multiple pregnancies necessitate meticulous prenatal care, with monochorionic pregnancies requiring close monitoring for TTTS.
From the 32nd week of gestation, weekly visits are recommended to observe fetal growth.
Childbirth Considerations
- Cesarean Delivery: Recommended for monochorionic-monoamniotic twins between 32–34 weeks, breech presentation, and significant fetal weight differences.
- Vaginal Delivery: Viable for diamniotic twins ≥ 32 0/7 weeks with one fetus in vertex presentation.
- Induction of Labor: Suggested for dichorionic-diamniotic twin pregnancies at 38 weeks' gestation.
Conclusion
The management of multiple pregnancies involves a nuanced understanding of their unique risks and complications. Through vigilant prenatal care and strategic delivery planning, many challenges can be navigated successfully, ensuring the well-being of both mother and fetuses.
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.