شرح المدرسين

Summary
Anemia during pregnancy is a significant global health concern. Distinguishing between physiologic anemia—a normal part of pregnancy due to increased plasma volume—and iron deficiency anemia is essential. It's also vital to identify and manage less common causes of anemia for the health of both the mother and child.
Definition of Anemia in Pregnancy
The World Health Organization (WHO) sets specific hemoglobin concentration thresholds for diagnosing anemia at different stages of pregnancy and postpartum, aiding in the identification and severity assessment of anemia:
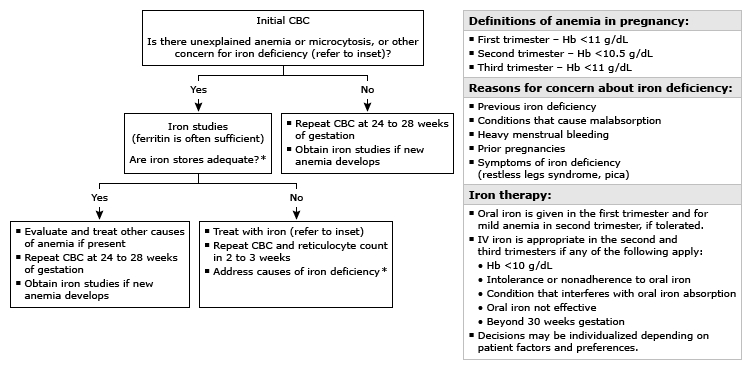
- First trimester: Hemoglobin <11 g/dL
- Second trimester: Hemoglobin <10.5 g/dL
- Third trimester: Hemoglobin <11 g/dL
- Postpartum: Hemoglobin <10 g/dL
Epidemiology and Health Care Disparities
An estimated 30% of reproductive-age women are anemic, with the prevalence rising to over 40% during pregnancy. The prevalence of anemia reflects socioeconomic and nutritional statuses, with higher rates in Black individuals due to factors including healthcare access and nutritional resources.
Causes of Anemia
- Physiologic (dilutional) anemia: A normal increase in plasma volume during pregnancy may result in mild anemia.
- Iron deficiency: The most common pathological cause of anemia in pregnancy, exacerbated by increased demands for fetal development and maternal blood volume expansion.
- Other causes: Include hemoglobinopathies, vitamin deficiencies (B12 and folate), and other inherited or acquired conditions.
Screening During Pregnancy
Screening for anemia with a complete blood count (CBC) is recommended at the first prenatal visit and again between 24 to 28 weeks. Individuals at high risk, such as those with previous iron deficiency diagnoses or certain chronic conditions, may need additional screening.
Prevention and Treatment of Iron Deficiency
Oral iron supplementation (27 to 30 mg daily) is recommended throughout pregnancy to meet increased iron demands. The treatment approach for diagnosed iron deficiency varies between oral and intravenous iron, based on anemia's severity, gestational age, and patient tolerance.
Diagnosis of Iron Deficiency Anemia (IDA)
IDA is characterized by reduced iron availability insufficient to meet the body's demands, particularly for erythropoiesis.
Laboratory Diagnosis
- Microcytosis: May suggest iron deficiency but is a late sign. Its presence or absence alone does not confirm or exclude IDA.
- Serum Ferritin: Essential for diagnosing iron deficiency.
- Levels below 30 ng/mL (<30 mcg/L) confirm iron deficiency.
- Levels ≥30 ng/mL generally exclude iron deficiency in those without comorbidities, though clinical judgment is essential.
Management Strategies
Management focuses on replenishing iron stores to correct anemia and prevent complications, varying by anemia's severity and pregnancy stage.
Initial Approach
- Oral Iron Supplementation: First-line treatment for IDA, effective and cost-efficient but may cause gastrointestinal side effects.
- Intravenous Iron: Used for severe anemia, oral iron intolerance, or when rapid iron repletion is necessary.
Key Considerations
- Safety: Both oral and intravenous iron treatments are safe during pregnancy, with intravenous iron reserved for the second and third trimesters.
- Efficacy: Aims to increase hemoglobin levels, improve maternal well-being, and support fetal development.
- Follow-up: Essential to monitor treatment response and ensure anemia resolution and iron store adequacy.
Management of Other Anemias
Tailor management based on the anemia's specific cause, including genetic counseling and treatments for conditions like sickle cell disease or thalassemia.
Postpartum Management
Continuing iron supplementation postpartum is recommended to replenish iron stores after delivery. Routine postpartum screening for anemia or iron deficiency is based on clinical judgment.
Conclusion
Anemia in pregnancy demands a nuanced approach to screening, diagnosis, and management. Tailored interventions based on individual risk factors and anemia type are crucial for optimal maternal and fetal health.
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.