سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Background
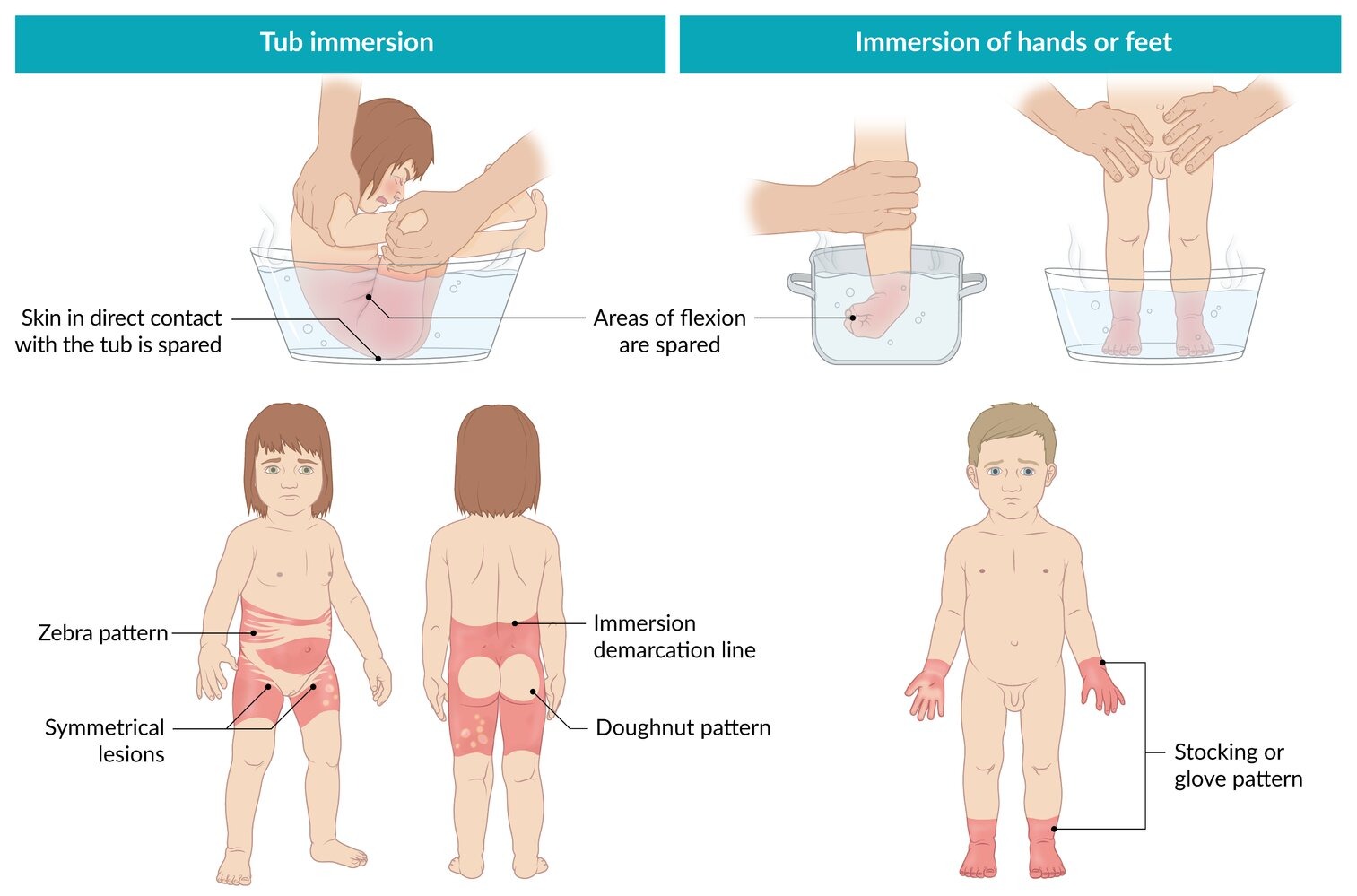
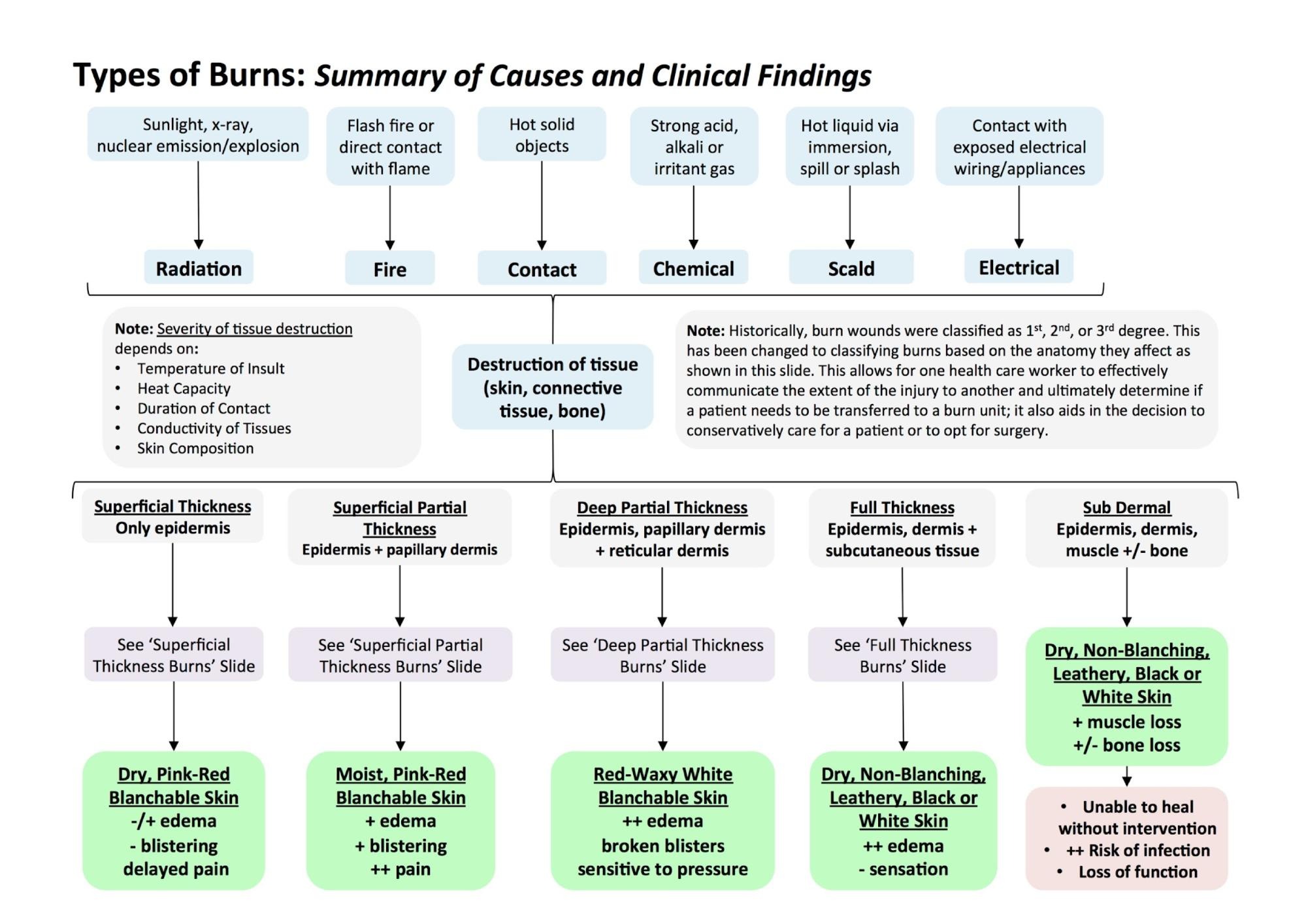
- Types of burn includes chemical (acid/alkali), electrical, radiation (UV, medical/therapeutic), thermal (scald, fire), and can be associated with abuse
- Most common causes in children are scald burns, while most common causes in adults are flame burns
- Early treatment for major burns include airway management, supplemental oxygen and large volumes of IV fluids
- All burns are initially managed with pain management, topical ointments and non-adherent dressing (major burns require debridement)
- Shock, sepsis and respiratory failure are among the most common cause of death after a burn injury

سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Etiology
- Thermal burns
- Most common type of burn
- Flame burns (fire)
- Contact burns (hot surfaces)
- Scalding (hot liquids or steam)
- Nonthermal burns
- Chemical burns
- Acids such as sulfuric acid, nitric acid, hydrofluoric acid, phenol, and acetic acid
- Alkalis such as calcium oxide, sodium hydroxide, and potassium hydroxide
- Electrical burns
- Low voltage sources: electrical cords, outlets in the households
- High voltage sources: power lines, lightening
- Radiation burns
- UV radiation (sunlight, phototherapy)
- High-energy particles (from radiotherapy, nuclear accidents)
- Friction burns
- Skin injury caused by abrasion against a hard surface
- Chemical burns
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Clinical presentation
| Classification | Degree | Site | Symptoms/Signs |
|---|---|---|---|
| Erythema/Superficial | 1st degree |
|
|
| Superficial-partial thickness | 2nd degree |
|
|
| Deep-partial thickness | 3rd degree |
|
|
| Full thickness | 4th degree |
|
|
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
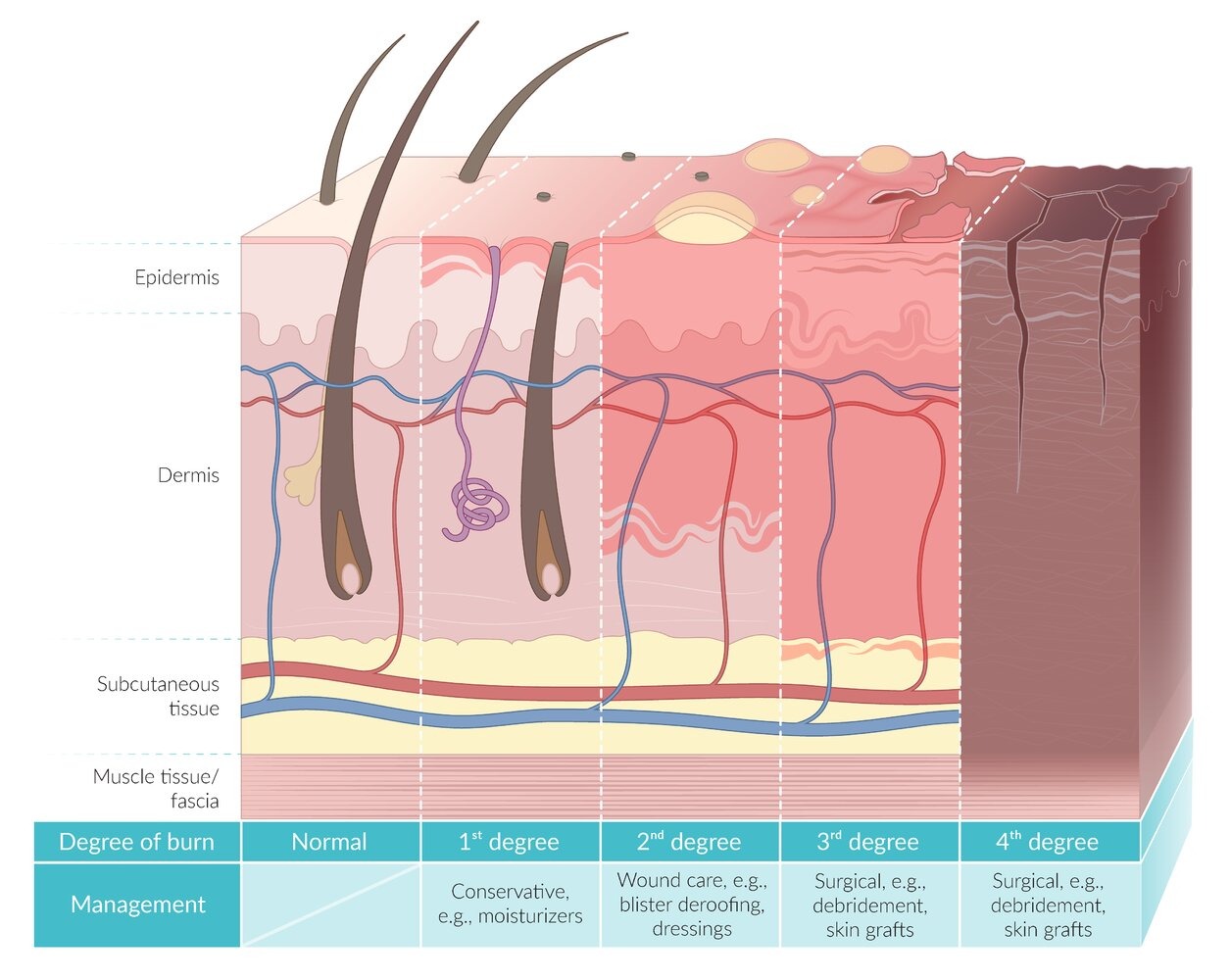
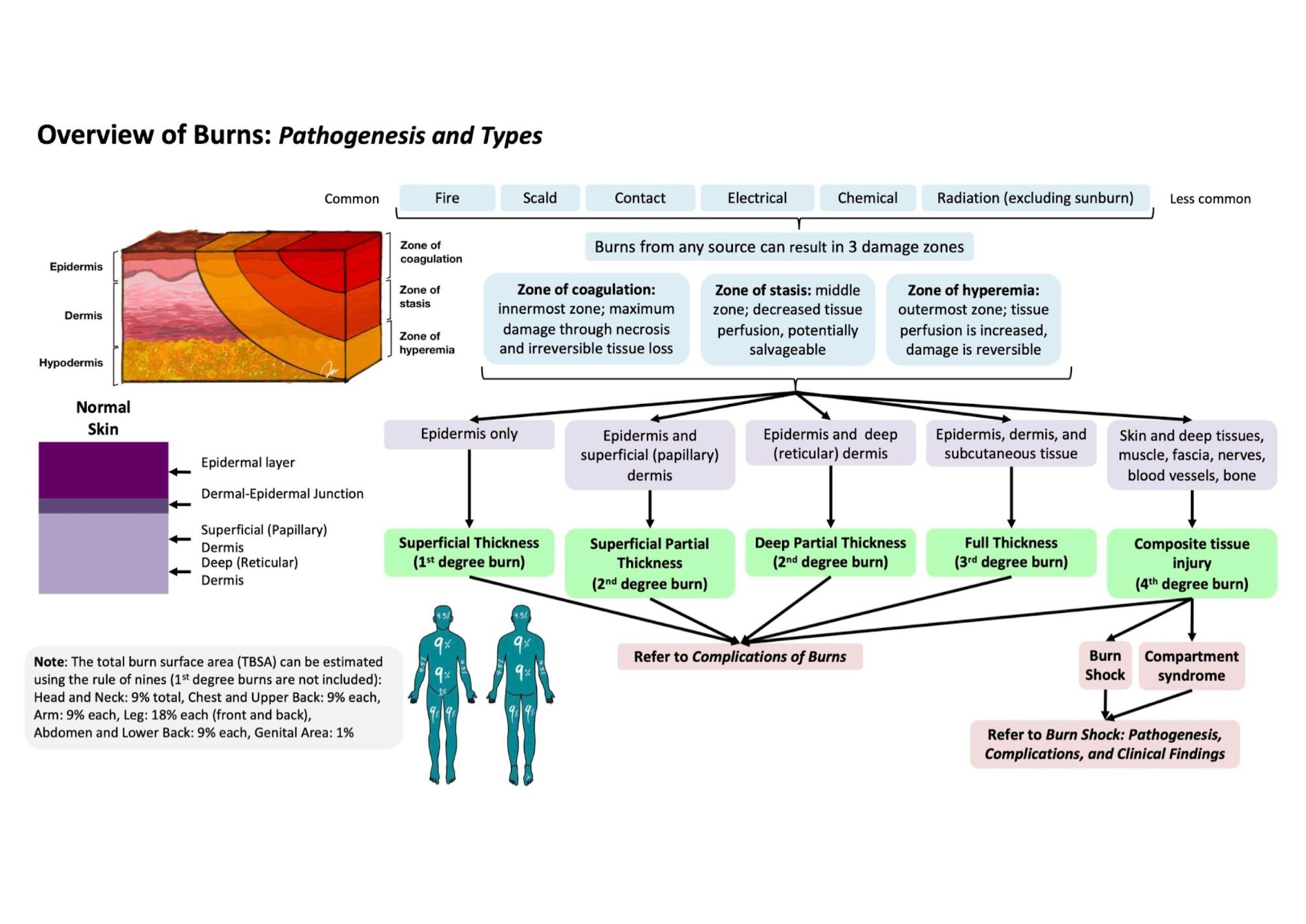
Burn Degrees
- 1st degree burn: superficial dermis
- Blanches on pressure and refills
- Healing within 3 to 6 days without scarring
- 2nd degree burn: dermis
- 2A blanches on pressure and refills
- 2B does not blanch on pressure
- Both have vesicles/bullae
- Healing takes 3 weeks or more, with hypopigmentation/hyperpigmentation
- 2B has scarring
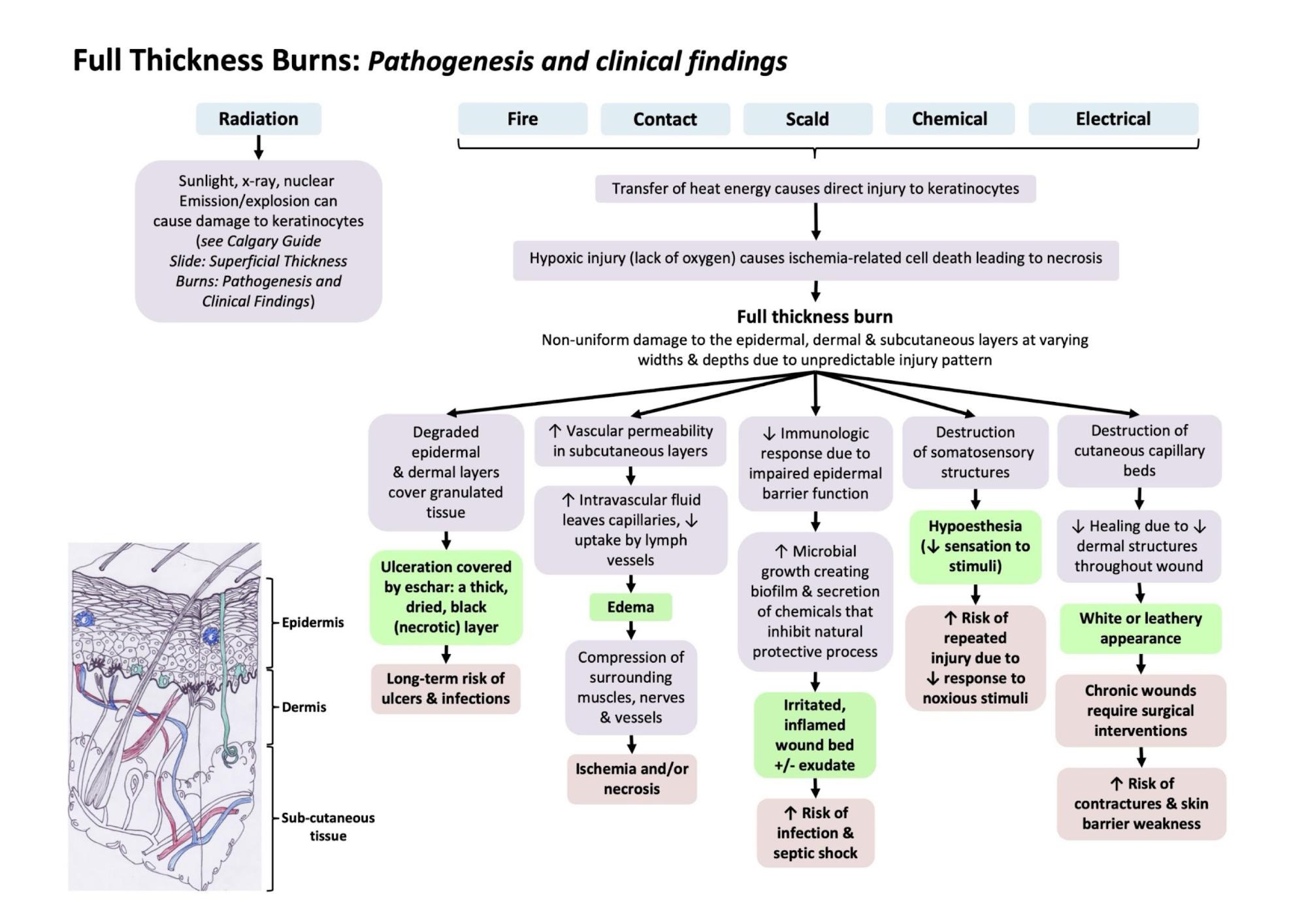
- 3rd degree burn: subcutaneous tissue
- No pain
- Black, white, leather like skin lesion (eschar)
- Does not heal by itself
- 4th degree burn: reaches muscle, fat, bone
- Charred tissue
- Dead tissue needs to be removed (amputation)
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
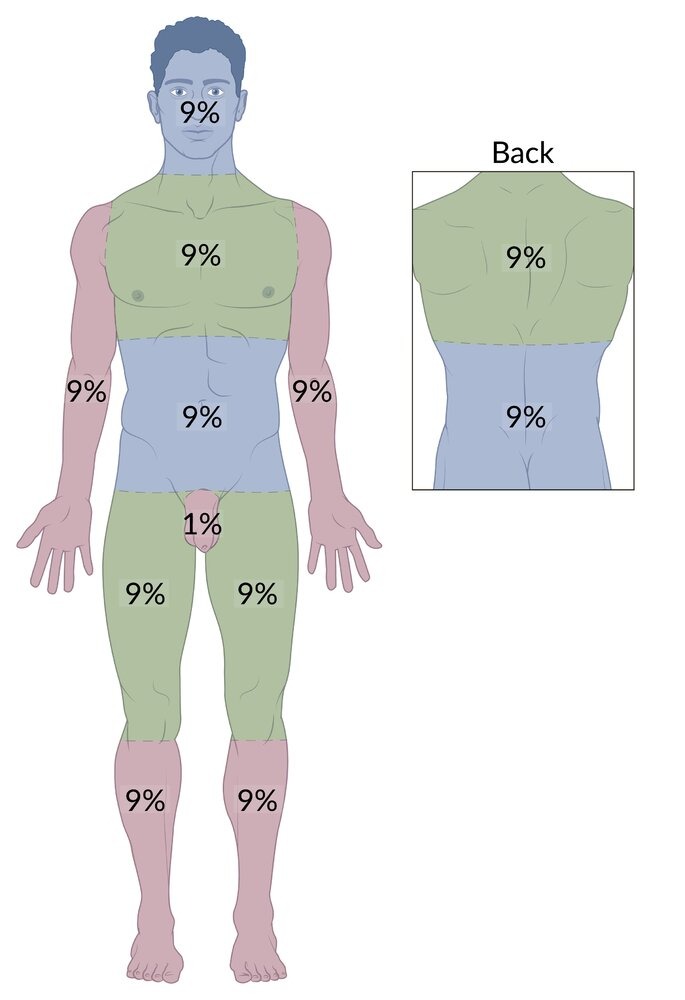
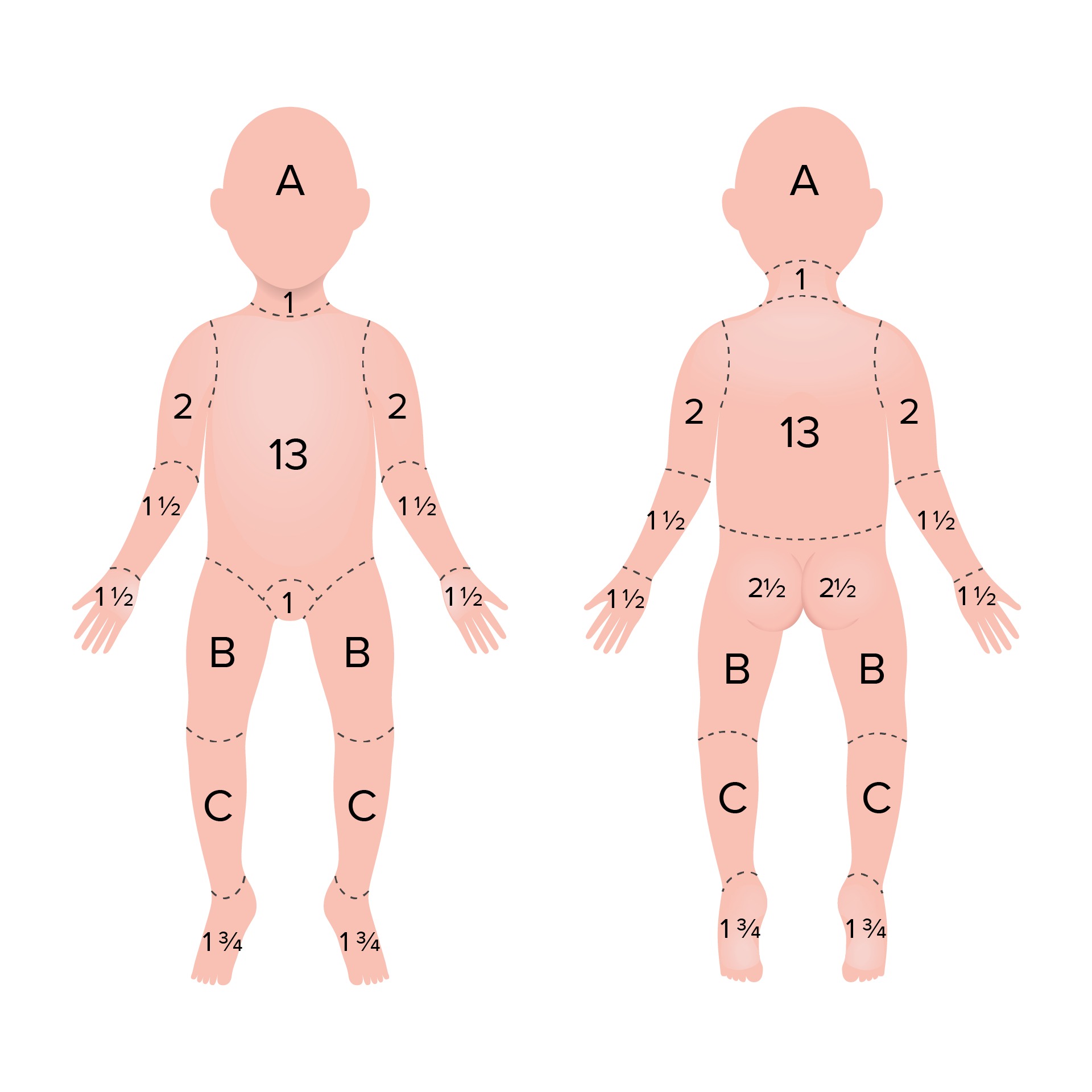
Rule of 9
- A clinical tool used to rapidly assess the TBSA affected by burns in adults
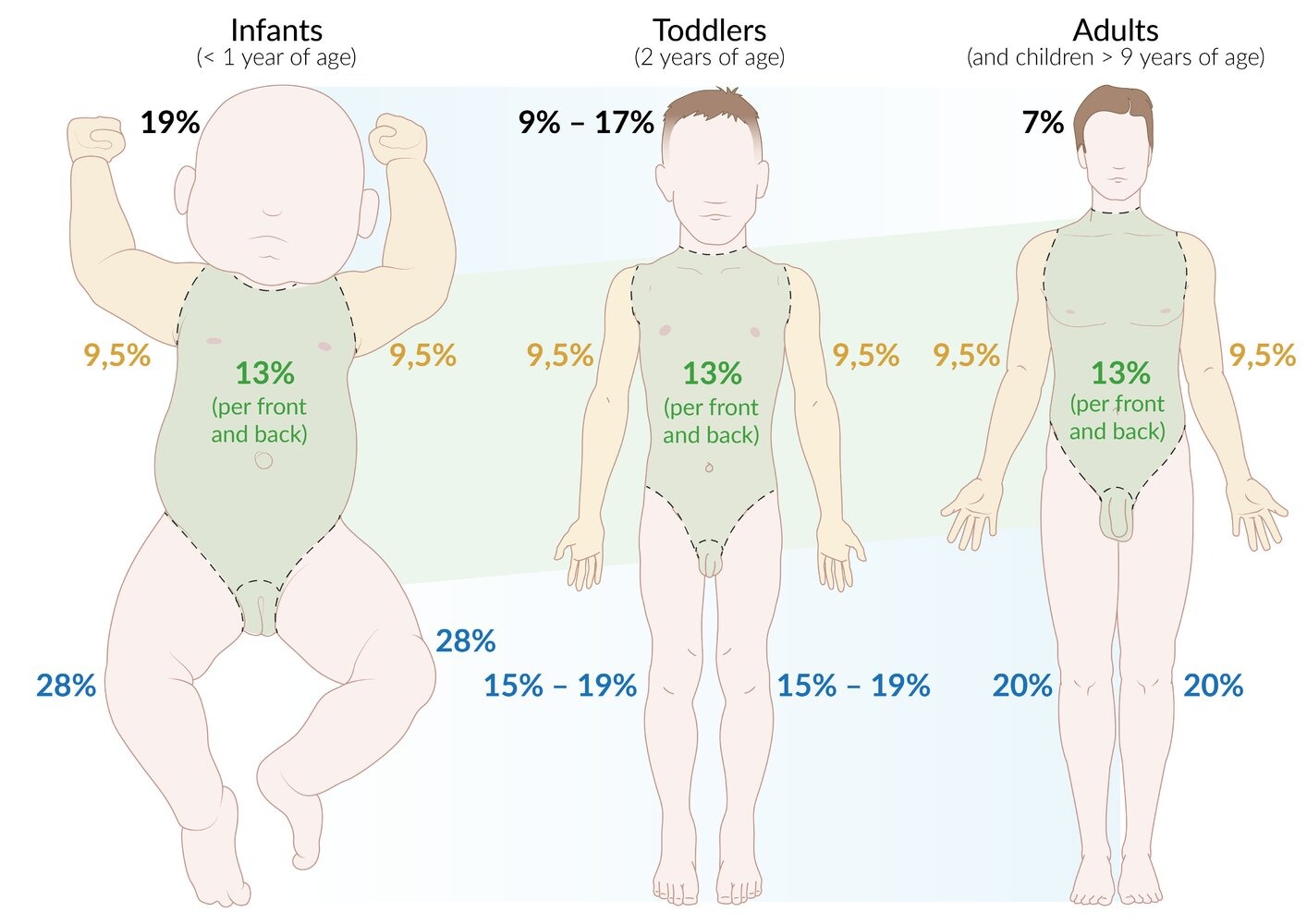
- The adult body is divided into regions (not children)
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Diagnosis
- Pulse oximetry or pulse CO-oximetry (to monitor for progressive hypoxemia, CO poisoning)
- Bronchoscopy (direct evaluation for possible airway injury that include mucosal edema, inhaled soot)
- Blood gas analysis
- Serum electrolytes
- ECG (to assess for arrhythmias for electrical injuries)
- Inhalational injury (respiratory function tests, chest X-ray, carboxyhemoglobin levels)
- Urinalysis (to distinguish myoglobinuria from hematuria)
- BUN/creatinine
- Hemoglobin and hematocrit
- Serum protein and albumin
- Wound swab and blood cultures
- Assessment of capillary refill and peripheral pulses if circumferential wounds
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Treatment
- ABCDE
- Fluid resuscitations
- Establish IV access
- Use lactated Ringer’s solution (to avoid hyperchloremic metabolic acidosis)
- Parkland formula (fluid resuscitation protocol for patients with burn injuries)
- 4 mL * Body weight (kg) * % of TBSA for the first 24 hours
- Local burn wound care (minor wounds)
- Acute pain management (acetaminophen or NSAIDs)
- Irrigate the wound to cool the area and remove the debris
- Clean the wound with soap or diluted
- Consider applying a topical antibiotics
- Consider non-adherent wound dressing if the skin is broken
- Local burn wound care (major wounds)
- Acute pain management (small frequent doses of IV opioids)
- Consider immediate escharotomy or fasciotomy if the limb perfusion is compromised
- Irrigate the wound to cool the area and remove the debris
- Clean the wound with soap or diluted
- Apply a topical antibiotics (bacitracin is used for partial-thickness burns, silver sulfadiazine is used for full thickness burns)
- Applying a wound dressing (occlusive dressing, hydrocolloid dressing, biosynthetic dressing)
- Definitive management
- Early debridement of necrotic tissue
- Wet-to-dry dressings for infected wounds or wounds with devitalized tissue
- Free skin grafts (eg, split thickness or full thickness skin graft)
- Burn reconstruction (eg, flap reconstruction with free or pedicled flaps)
| Hypermetabolic Response in Burn Injury | |
|---|---|
| Etiology |
|
| Clinical Features |
|
| Treatment |
|
| Criteria to Transfer to Burn Center |
|---|
|
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
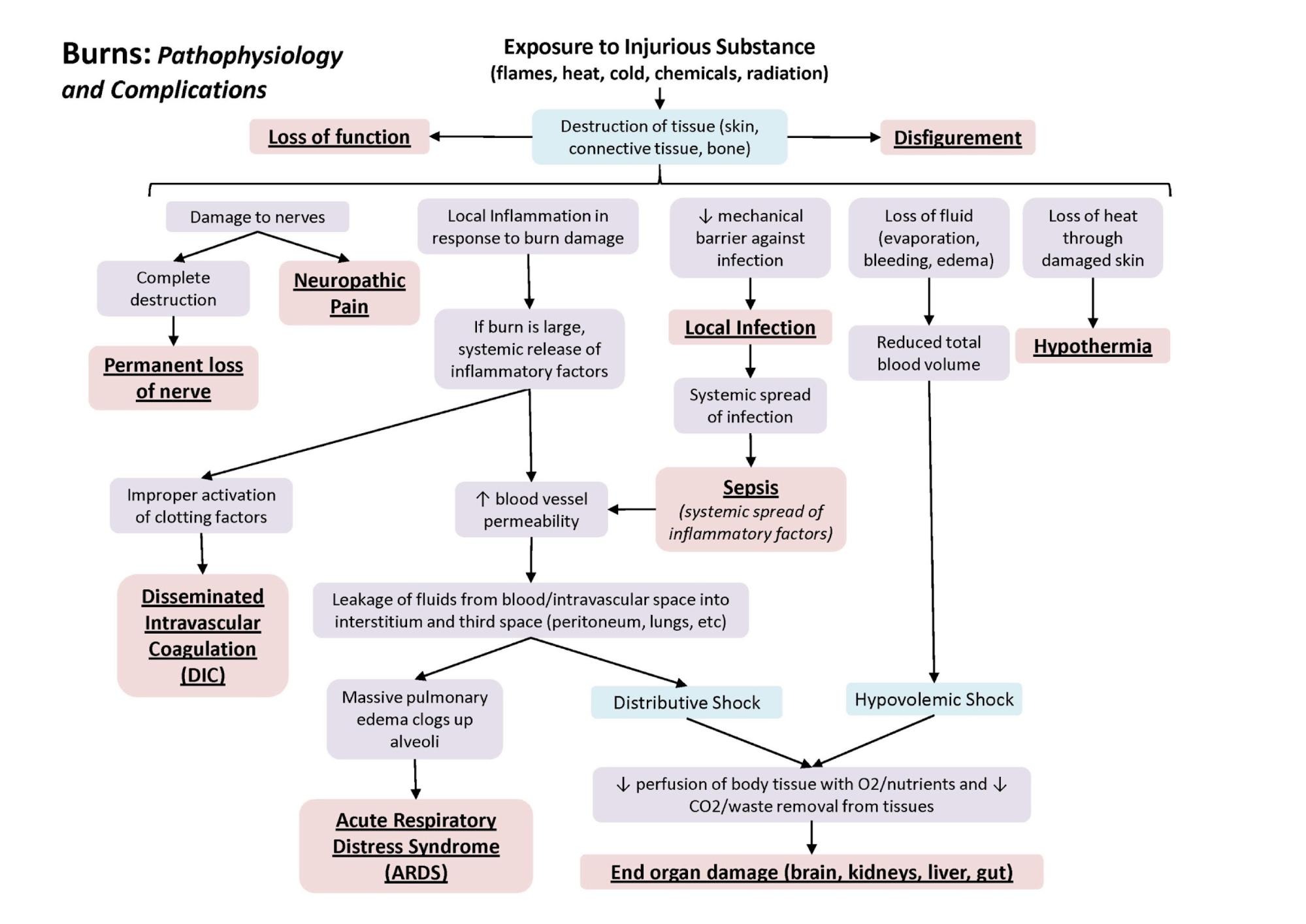
Complications
- Shock, sepsis and respiratory failure
- Most common causes of death from burns
- Common organisms of sepsis include MRSA, enterococcus and Pseudomonas
- Circumferential burns may lead to
- Compartment syndrome
- Acute limb ischemia
- Curling ulcers
- Keloid formation, contractures
- Marjolin ulcer
- Complications of chemical burns
- Cataracts or vision loss (if the burn involves the eyes)
- Esophageal strictures (if the burn involves the esophagus)
- Complications of electrical burns
- Arrhythmias
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.
فيديوهات الشرح
بطاقات تفاعلية
أسئلة ممارسة
اشترك الآن