Summary
Gallstones (cholelithiasis) represent the most common biliary pathology, affecting 10-20% of adults in developed countries. These crystalline deposits form within the gallbladder through precipitation of bile constituents - primarily cholesterol (75%) or bilirubin. While most gallstones remain asymptomatic, approximately 20-30% will eventually cause symptoms, most commonly biliary colic - episodic RUQ pain lasting <6 hours triggered by fatty meals.
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Definition
- Cholelithiasis: Formation of stones within the gallbladder
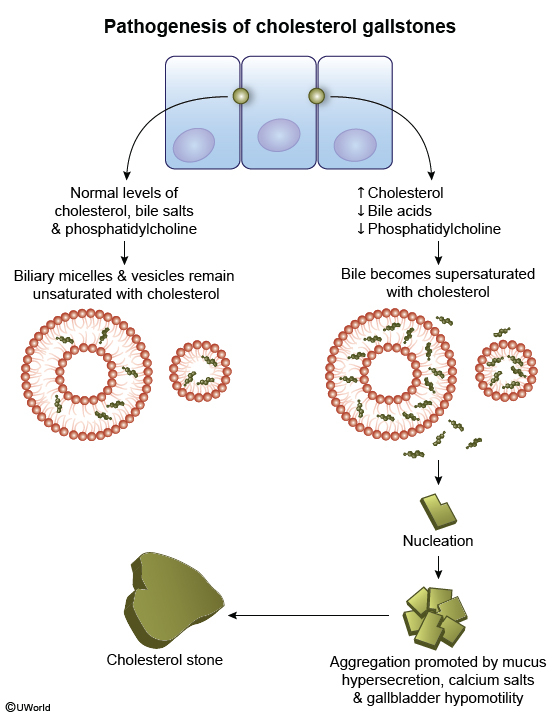
- Pathophysiology: Imbalance between cholesterol/bilirubin and solubilizing factors (bile salts, lecithin) → precipitation → stone formation
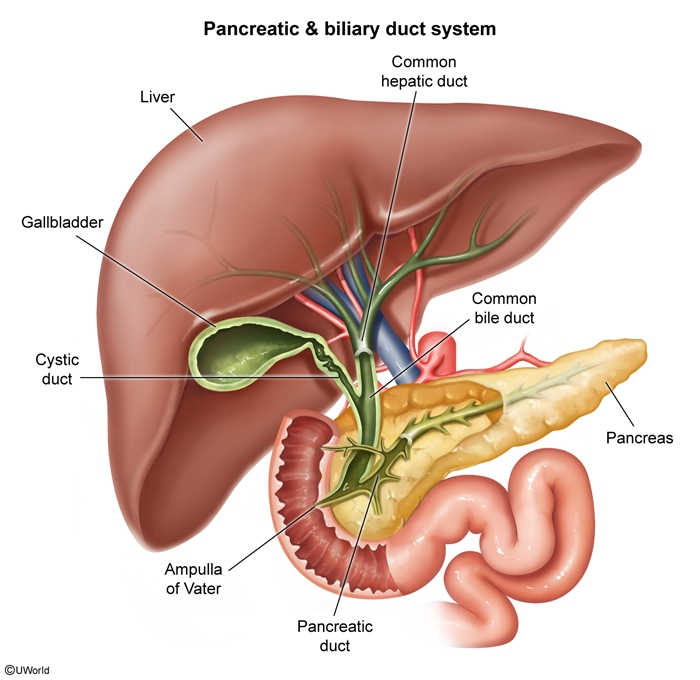
- Location:
- Gallbladder (cholelithiasis) - most common
- Common bile duct (choledocholithiasis)
- Intrahepatic ducts (rare)
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Epidemiology
- Prevalence: 10-20% of adults in developed countries
- Gender: Female > Male (2-3:1)
- Age: Increases with age, especially after 40 years
- Geography: Higher in Western countries, Native Americans, Hispanics
- Risk factors mnemonic: The 6 F's
- Fat (obesity)
- Female
- Fertile (multiparity)
- Forty (age > 40)
- Fair-skinned
- Family history
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
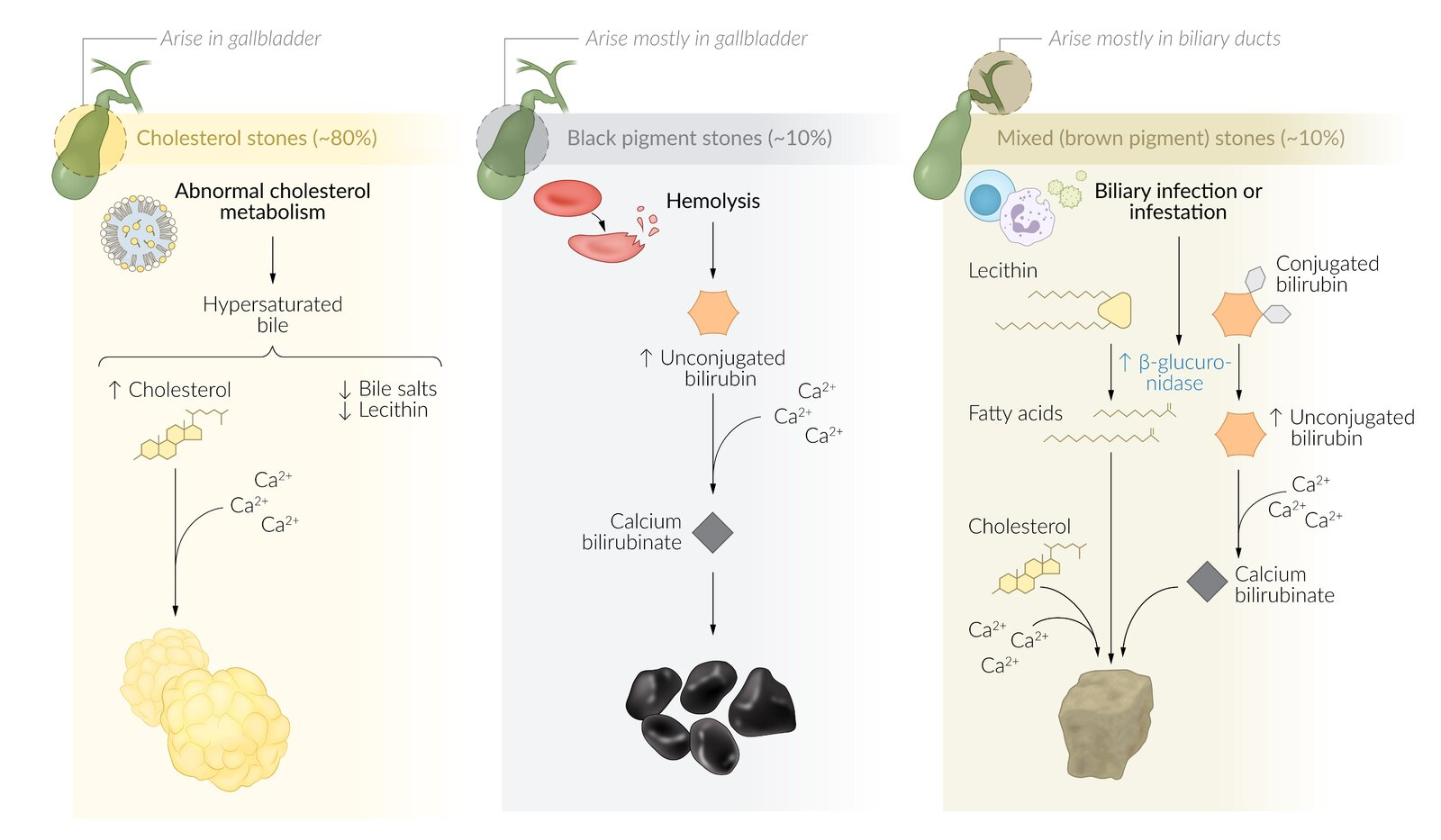
Types of Gallstones
- Cholesterol stones (80%)
- Pure cholesterol: ~10%, single, large, yellow
- Mixed stones: ~70%, multiple, contain cholesterol + calcium salts
- Risk factors: obesity, female sex, pregnancy, drugs (fibrates, OCPs)
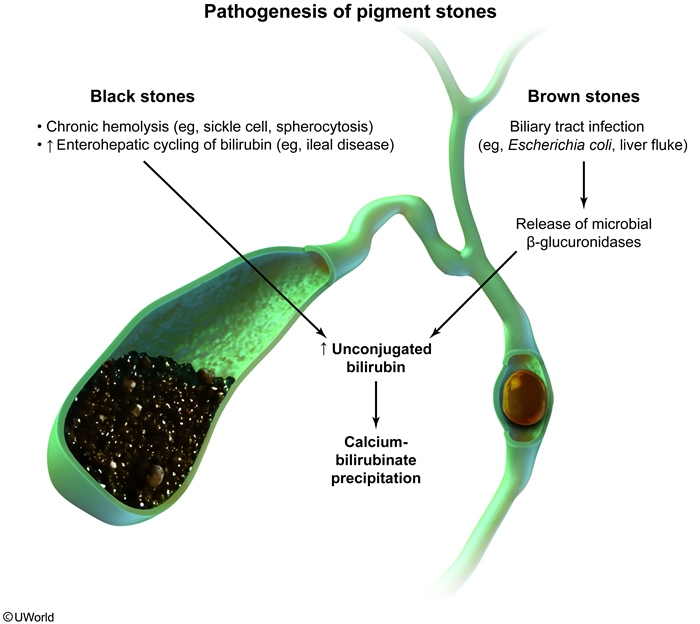
- Pigment stones (20%)
- Black pigment stones:
- Calcium bilirubinate polymers
- Associated with hemolysis (sickle cell, thalassemia)
- Also seen in cirrhosis
- Brown pigment stones:
- Calcium bilirubinate + fatty acids
- Associated with infections (E. coli, parasites)
- Common in Asia
- Black pigment stones:
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Etiology / Risk Factors
- Cholesterol Stones
- Increased cholesterol secretion:
- Obesity, high-fat diet
- Pregnancy, estrogen therapy, OCPs
- Genetics (ABCG5/G8 mutations)
- Decreased bile acids:
- Terminal ileal disease/resection
- Cholestyramine use
- Fibrates (inhibit cholesterol 7α-hydroxylase)
- Gallbladder stasis:
- Pregnancy, TPN, rapid weight loss
- Octreotide, fasting
- Vagotomy, diabetes
- Increased cholesterol secretion:
- Black Pigment Stones
- Composed of calcium bilirubinate polymer + calcium salts
- Chronic hemolysis → ↑ unconjugated bilirubin
- Cirrhosis → ↓ bilirubin conjugation
- Gilbert syndrome
- Brown Pigment Stones
- Made of calcium bilirubinate, palmitate, and stearate, often mixed with cholesterol
- Most common in Asia; form in ducts due to infection
- β‑glucuronidase from bacteria (E. coli, Klebsiella) deconjugates bilirubin → precipitation → stone formation
- Associated with bile stasis, infection, stents, parasites (Clonorchis, Ascaris)
| Important – فكرة سؤال | |
| Remember: Cholesterol stones are radiolucent (not seen on X-ray), while only 15-20% of stones are radiopaque. This is why ultrasound is preferred over X-ray for diagnosis. | تذكر |
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Clinical Presentation
- Asymptomatic (70-80%)
- Incidental finding on imaging
- Annual risk of symptoms: 1-2%
- Usually no treatment needed
- Biliary colic (20-30%)
- Pain characteristics:
- Nocturnal, constant, NOT colicky (despite the name)
- RUQ or epigastric pain
- Radiation to right shoulder/scapula
- Duration: 30 min - 6 hours
- Triggers: Fatty meals, large meals
- Associated symptoms: Nausea, vomiting
- Physical exam: RUQ tenderness, no fever
- Pain characteristics:
| Note | |
| If pain lasts > 6 hours, think complications (acute cholecystitis). If fever is present, it's NOT simple biliary colic. | ملاحظة |

سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Diagnosis
- Laboratory tests
- Usually NORMAL in uncomplicated cholelithiasis
- CBC, LFTs, amylase/lipase → to rule out complications
- Imaging
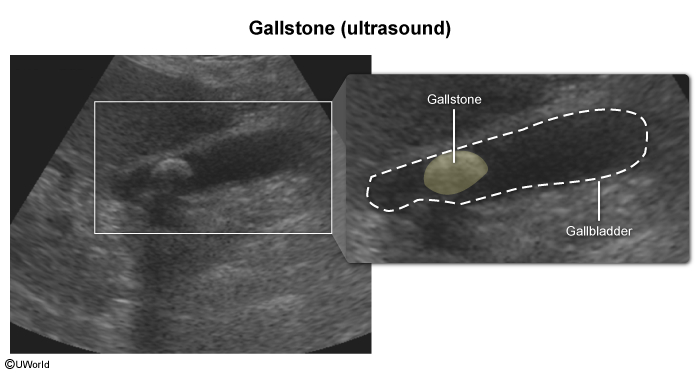
- RUQ Ultrasound (first-line):
- Sensitivity > 95% for stones > 2mm
- Shows hyperechoic foci with acoustic shadowing
- Can detect sludge and GB wall thickening
- CT scan:
- Poor for gallstones (only 15-20% are radiopaque)
- Better for complications
- MRCP:
- If ultrasound inconclusive
- Excellent for CBD stones
- RUQ Ultrasound (first-line):
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Management
- Asymptomatic gallstones
- Expectant management (observation)
- Prophylactic cholecystectomy ONLY if:
- Porcelain gallbladder
- Gallstones ≥ 3 cm
- Gallbladder polyps ≥ 1 cm
- Planning bariatric surgery
- Chronic hemolytic anemia (children)
- Symptomatic gallstones
- Acute management:
- NSAIDs (ketorolac) - first line
- Opioids if NSAIDs contraindicated
- Antiemetics, IV fluids
- Definitive treatment:
- Laparoscopic cholecystectomy = GOLD STANDARD
- Timing: elective, within 6 weeks
- Acute management:
- Non-surgical options (if surgery contraindicated)
- Ursodeoxycholic acid
- Only for small (<1cm), radiolucent stones
- Success rate: 30-50%
- High recurrence (50% at 5 years)
- Ursodeoxycholic acid
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Complications
- Acute cholecystitis: Persistent cystic duct obstruction → inflammation → fever + Murphy sign
- Choledocholithiasis: CBD stone → jaundice + ↑ ALP/bilirubin
- Cholangitis: CBD obstruction + infection → Charcot triad (pain + fever + jaundice)
- Biliary pancreatitis: Stone at ampulla → ↑ lipase/amylase
- Gallstone ileus: Fistula → bowel obstruction (rare)
- Mirizzi syndrome: Cystic duct stone compressing CHD
- Gallbladder cancer: Rare (< 1%)
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Summary Table
| Gallstones - Quick Review | |
|---|---|
| Prevalence | 10-20% adults; F:M = 2-3:1; ↑ after 40 years |
| Risk factors | 6 F's: Fat, Female, Forty, Fertile, Fair, Family history |
| Types | Cholesterol (80%), Black pigment, Brown pigment |
| Presentation | 70% asymptomatic; Biliary colic: RUQ pain < 6h after fatty meal |
| Diagnosis | RUQ ultrasound (first-line); Labs usually normal |
| Treatment | Symptomatic → Laparoscopic cholecystectomy |
| Complications | Cholecystitis, choledocholithiasis, cholangitis, pancreatitis |
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.
فيديوهات الشرح
بطاقات تفاعلية
أسئلة ممارسة
اشترك الآن