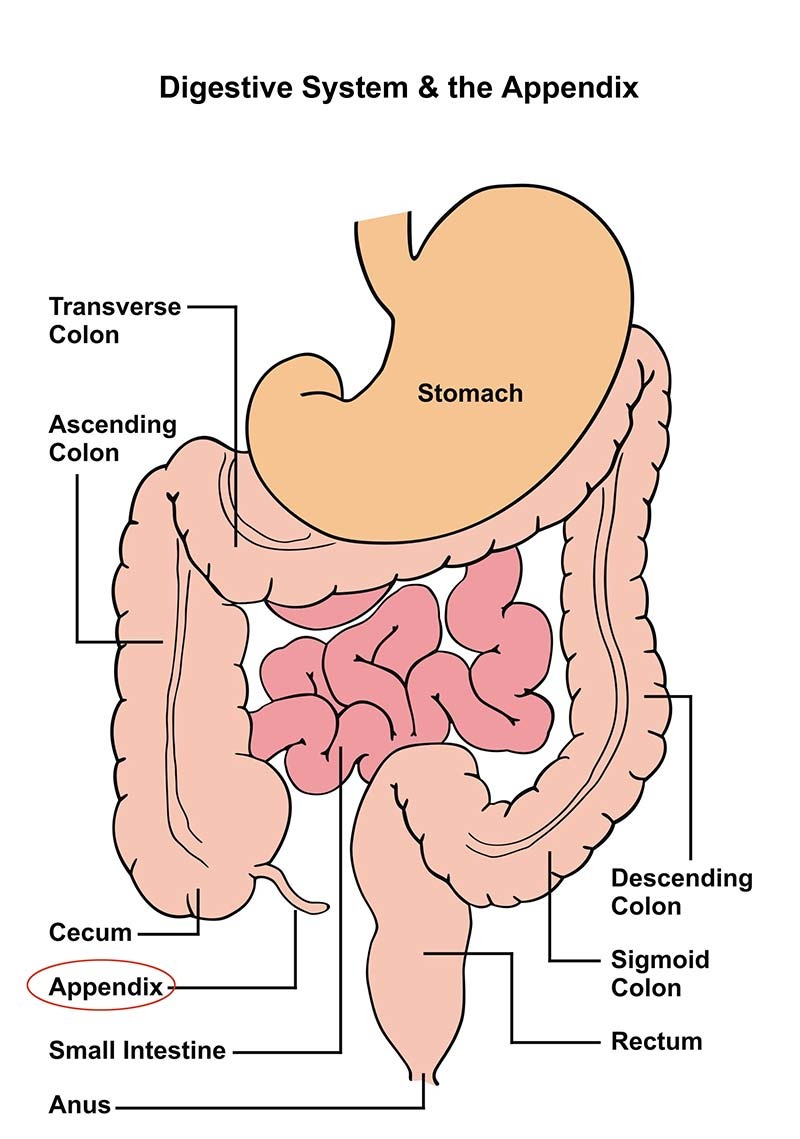
Definition
Appendicitis is an acute inflammation of the vermiform appendix, typically due to luminal obstruction. Most common cause of acute abdomen requiring emergency surgical intervention.
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Background
- Definition: Acute inflammation of the appendix.
- Most commonly caused by obstruction of the appendiceal lumen:
- Fecalith in adults
- Lymphoid follicular hyperplasia in children
- Obstruction leads to increased intraluminal pressure, causing visceral (periumbilical) pain initially.
- As inflammation worsens and irritates the parietal peritoneum, pain localizes to the right lower quadrant (RLQ).
- Definitive treatment is appendectomy.
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
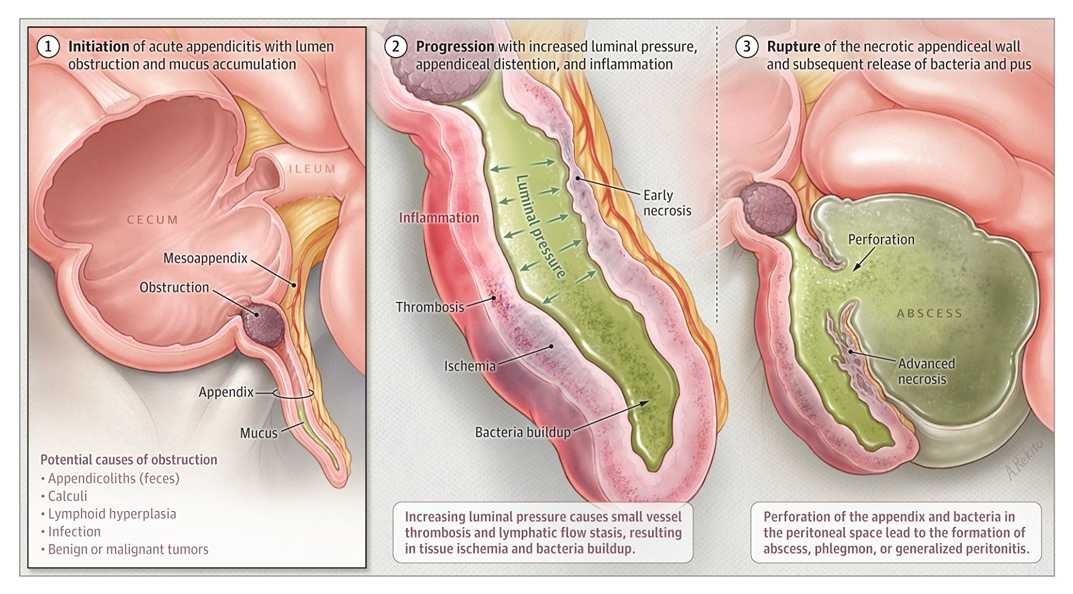
Pathophysiology
- Primary mechanism: Luminal obstruction → ↑ intraluminal pressure → bacterial overgrowth → inflammation → potential perforation
- Adults: fecaliths most common
- Children: lymphoid hyperplasia most common
- Other less common causes: tumors, parasites, foreign bodies
- Clinical progression:
- Early stage (0–12 h): Visceral, periumbilical pain
- Middle stage (12–24 h): Localized RLQ pain (parietal peritoneum involvement)
- Late stage (>24 h): ↑ risk of perforation & generalized peritonitis
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Clinical Features
- Pain pattern:
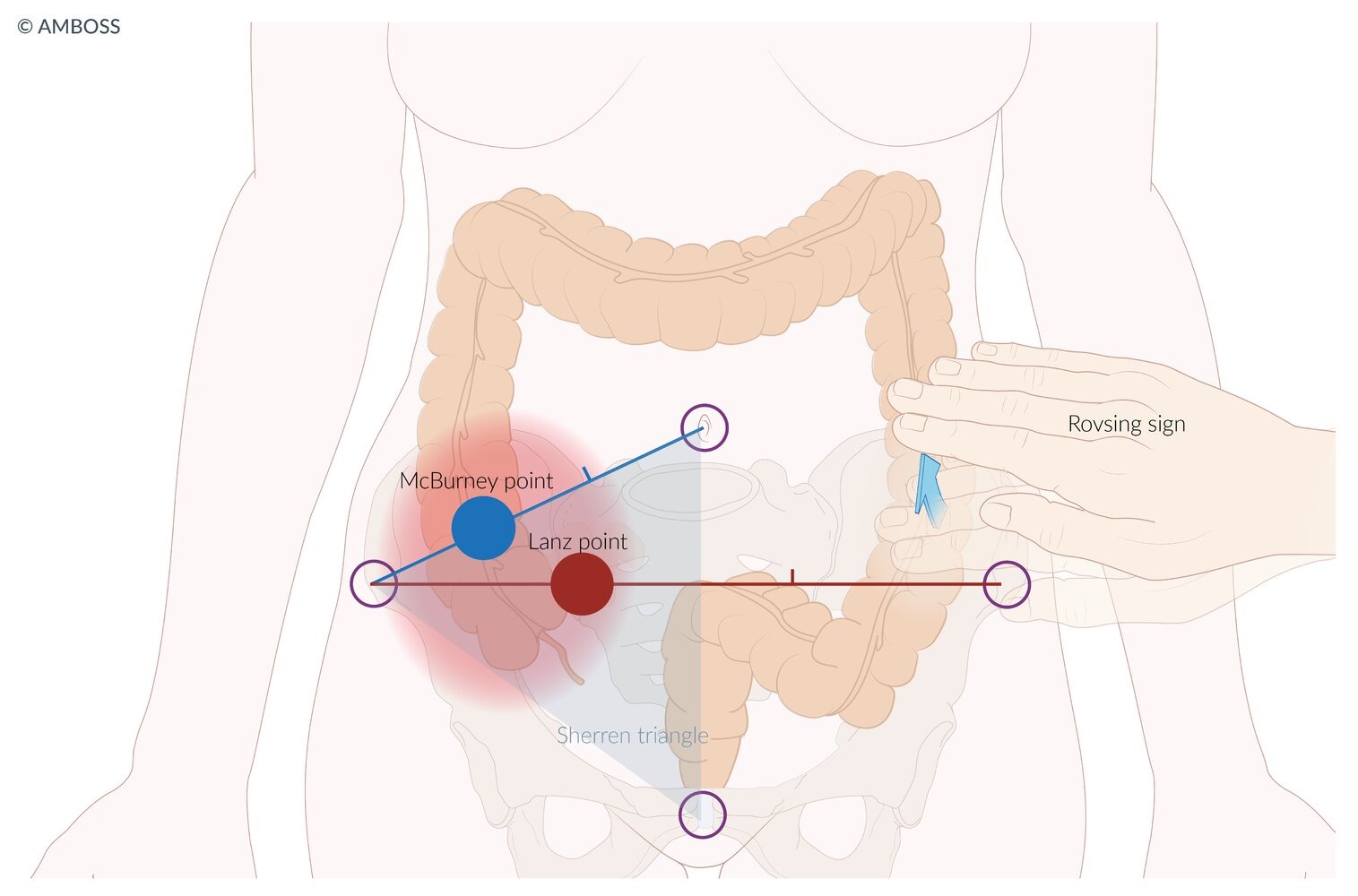
- Initial periumbilical discomfort → migrates to RLQ (McBurney’s point)
- Worsened by movement, coughing
- Nausea/vomiting often follows onset of pain
- Anorexia: Very common, frequently the earliest symptom
- Fever: Typically low-grade; high fever raises suspicion for perforation
- Physical exam:
- McBurney’s point tenderness (most sensitive)
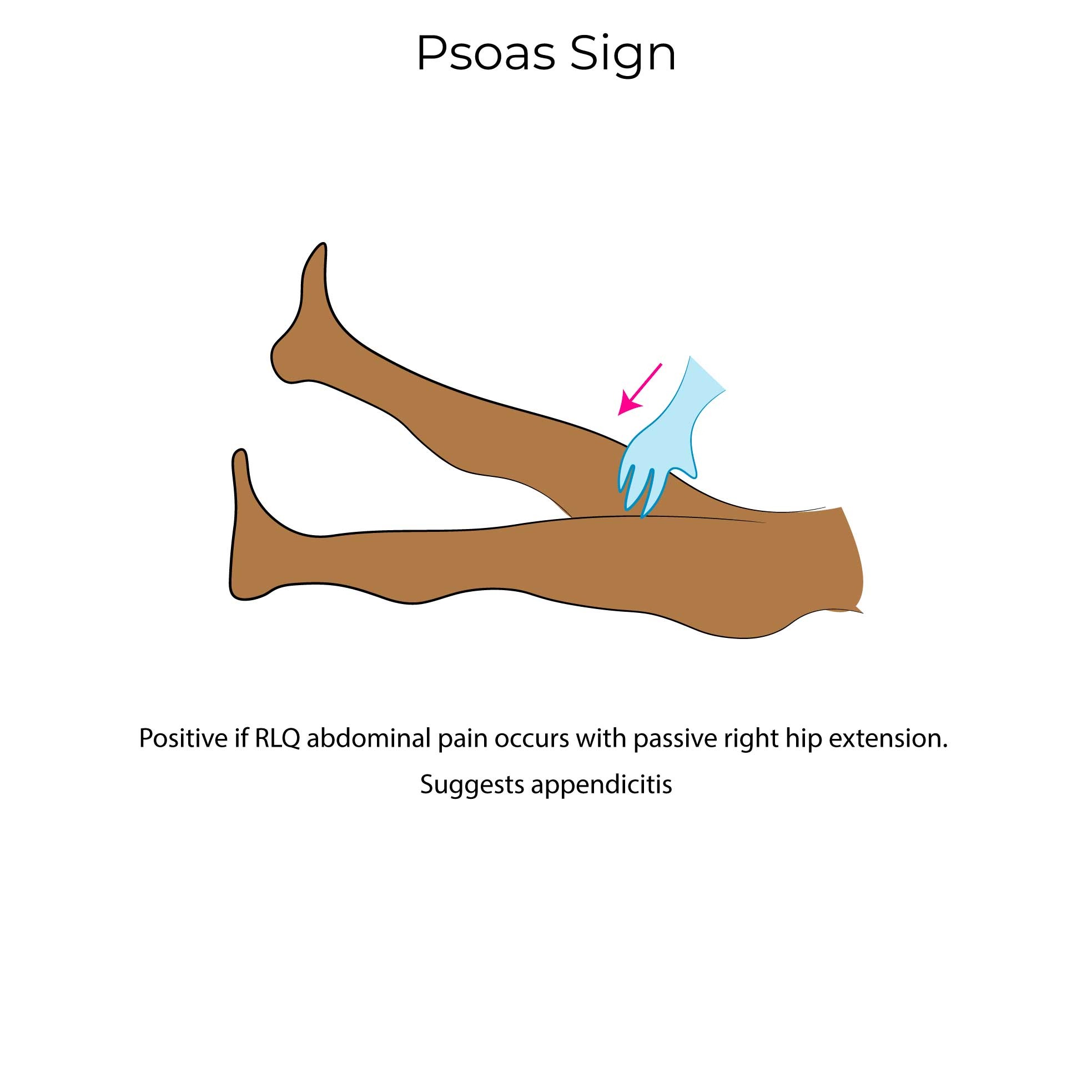
- Rovsing’s sign, Psoas sign, Obturator sign
- Rebound tenderness, guarding, rigidity → signs of peritoneal irritation
- Atypical presentations:
- Elderly: vague symptoms, often late presentation, higher perforation risk
- Pregnancy: appendix displaced upward, can present with RUQ or flank pain
- Retrocecal appendix: back/flank pain, minimal abdominal findings
- Pelvic appendix: suprapubic pain, urinary symptoms, rectal tenderness
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Diagnostics
- Laboratory tests:
- CBC with differential: Leukocytosis (>10,000/μL), left shift
- CRP, ESR: Elevated in most cases
- Urinalysis: Typically normal (mild WBC/RBC possible but not significant)
- β-hCG in women of childbearing age to rule out ectopic pregnancy
- Imaging:
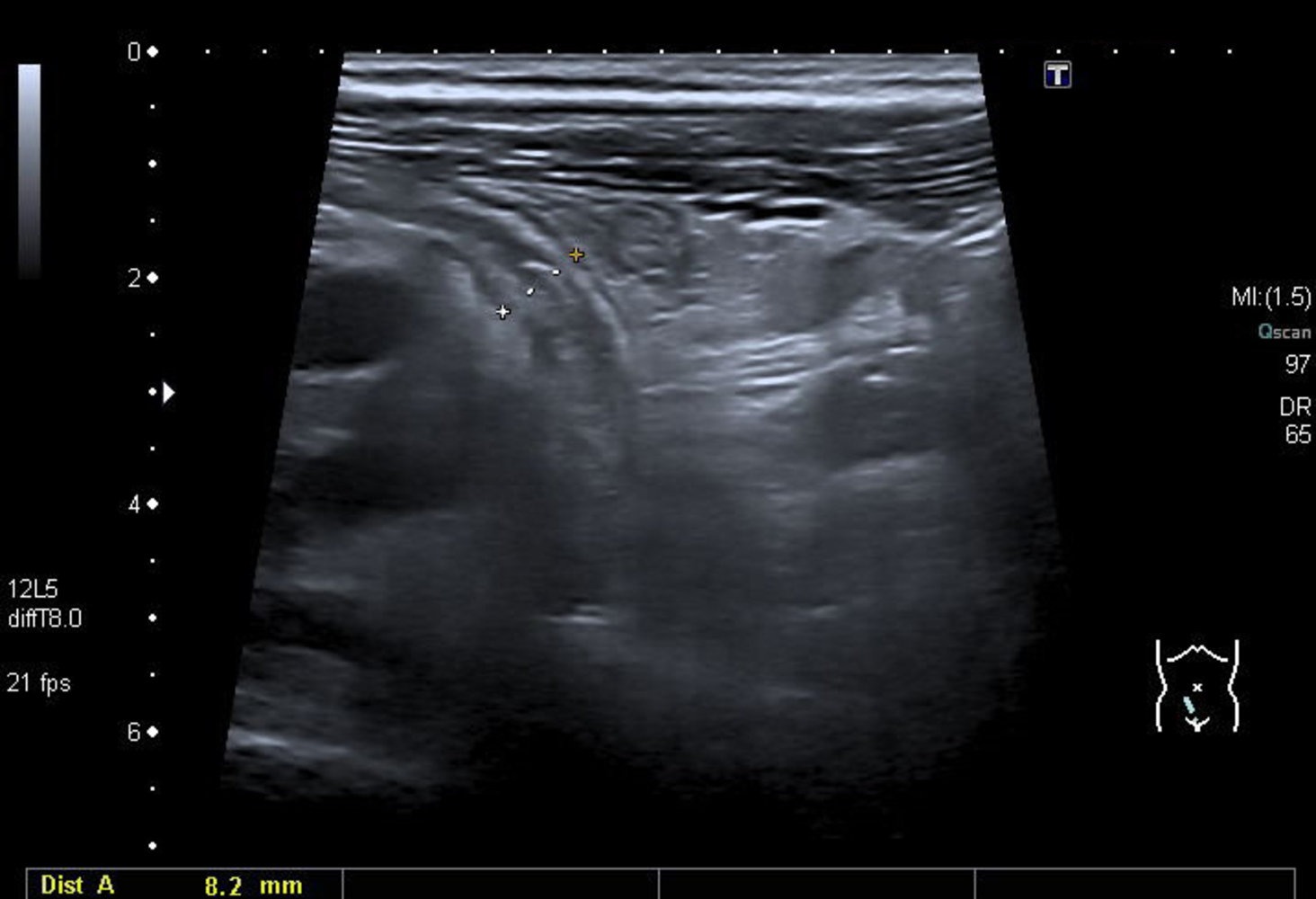
- Ultrasound: First-line in children/pregnancy
- Non-compressible appendix >6 mm, target sign, periappendiceal fluid
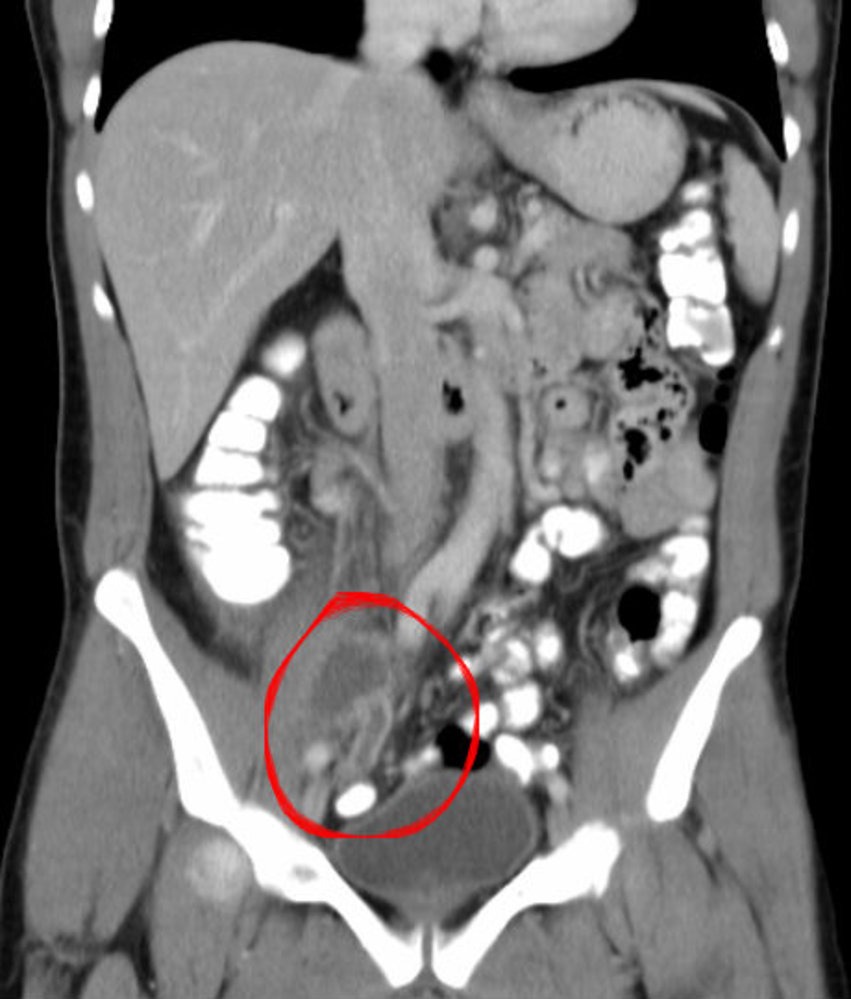
- CT Abdomen/Pelvis (with contrast): Gold standard in adults
- Appendix >6 mm, wall thickening, fat stranding, ± appendicolith
- Ultrasound: First-line in children/pregnancy
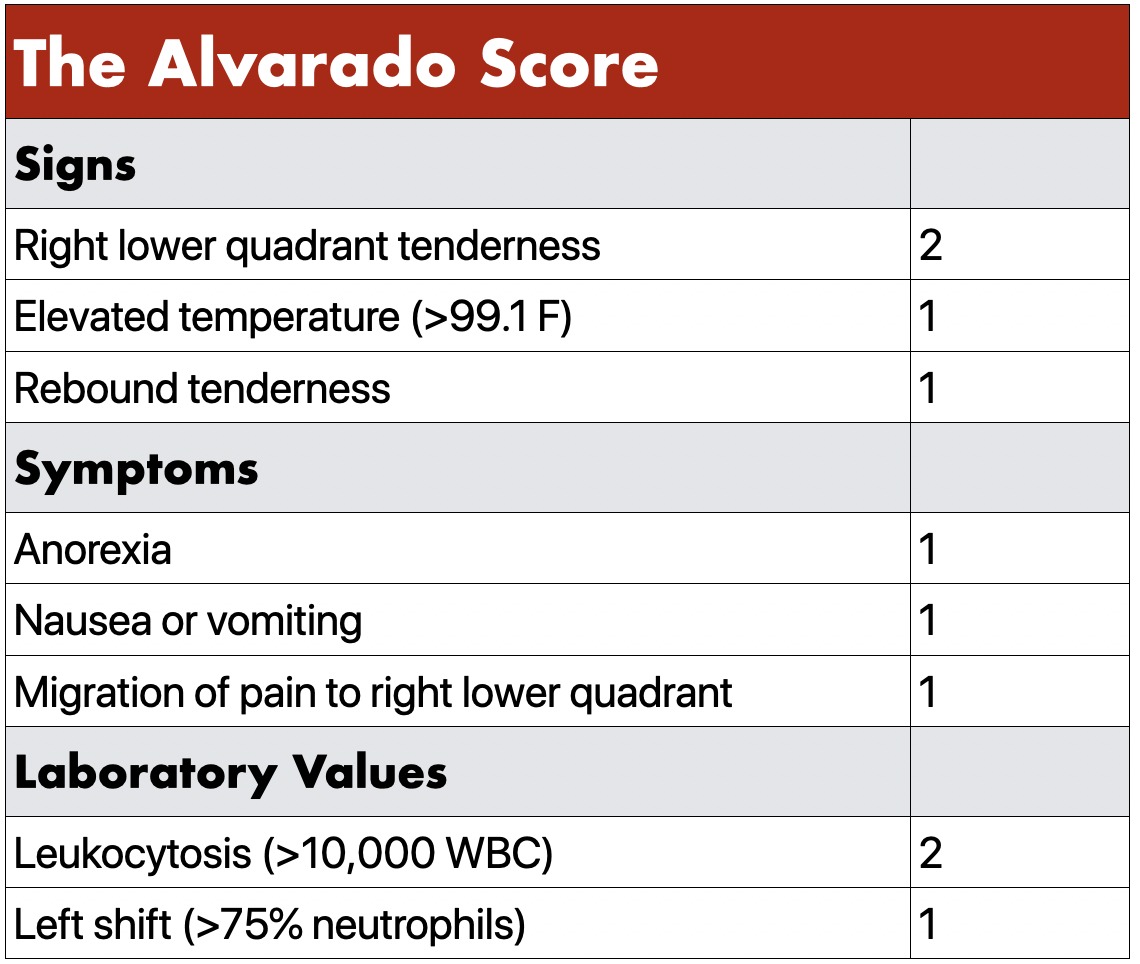
- Alvarado score: clinical tool based on symptoms, exam findings, labs
- ≥7: high probability
- 5–6: intermediate
- ≤4: low probability

سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Examination Signs in Appendicitis
| Sign | Findings | Significance |
| Peritoneal Signs (Rebound Tenderness, Guarding, Rigidity) |
|
|
| Psoas Sign |
|
|
| Obturator Sign |
|
|
| Rovsing’s Sign |
|
|
| Rectal Tenderness |
|
|
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Alvarado Score
- A clinical scoring system used to assess the likelihood of acute appendicitis.
- Components:
- Migration of pain (1 point)
- Anorexia (1 point)
- Nausea/vomiting (1 point)
- RLQ tenderness (2 points)
- Rebound pain (1 point)
- Fever (1 point)
- Leukocytosis (2 points)
- Left shift (1 point)
- Interpretation:
- ≥7: High probability
- 5-6: Intermediate
- ≤4: Low probability
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Treatment
- Initial management: NPO, IV fluids, analgesics, antiemetics, and antibiotics if indicated
- Antibiotics:
- Simple (uncomplicated): Cefoxitin or Ceftriaxone + Metronidazole
- Complicated: Broad-spectrum regimens (e.g., Piperacillin-tazobactam)
- Definitive treatment:
- Surgery: Laparoscopic appendectomy (preferred) within 12–24 hours
- Non-operative management: Selected uncomplicated cases (antibiotics only); ~40% recurrence rate at 5 years
- Complicated cases (e.g., perforation, abscess):
- Emergency surgery if diffuse peritonitis or sepsis
- Percutaneous drainage (abscess >3 cm)
- Extended antibiotic coverage
- Interval appendectomy (6–8 weeks) sometimes considered
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Complications
- Perforation: ~36–48 hours after onset if untreated, leading to peritonitis
- Abscess formation: may require drainage and prolonged antibiotics
- Other: Adhesions, bowel obstruction, pylephlebitis
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Differential Diagnosis
- Ectopic pregnancy
- Pseudoappendicitis
- Meckel diverticulum
- Diverticulitis (especially in elderly patients)
- Psoas abscess (in patients with a positive psoas sign)
- Inflammatory bowel disease
- Gastroenteritis
- Colon cancer
- Urolithiasis and renal colic
- Urinary tract infections
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Prognosis
- Mortality in uncomplicated appendicitis <0.1%
- Perforated cases: mortality ~0.6%, but higher in elderly
- Negative appendectomy rate: 10–15%
- Recovery: 1–3 weeks depending on technique and complications
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Psoas abscess
| Psoas Abscess | |
| Clinical Presentation |
|
| Diagnosis |
|
| Treatment |
|
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Diverticular disease
| Diverticular Disease | |
| Etiology |
|
| Symptoms |
|
| Risk Factors |
|
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.
فيديوهات الشرح
بطاقات تفاعلية
أسئلة ممارسة
اشترك الآن