Summary
Upper Respiratory Tract Infections (URTIs) are the most common acute illnesses in children. They involve the nose, sinuses, pharynx, tonsils, and larynx, and most are caused by viruses (rhinovirus, RSV, adenovirus, parainfluenza, influenza).
Children typically get 6–8 episodes per year, especially those in daycare or with school-age siblings. Most are self-limiting and need only supportive care.
This lesson covers the main URTI syndromes seen on the SMLE/internship exam:
- Common cold (viral nasopharyngitis)
- Pharyngitis / tonsillitis — viral vs Group A Strep (GAS)
- Acute otitis media (AOM)
- Acute rhinosinusitis
- Croup (laryngotracheobronchitis)
- Epiglottitis
- Bacterial tracheitis
The three "stridor + fever" emergencies — croup, epiglottitis, and bacterial tracheitis — are the highest-yield differentials and are compared side-by-side at the end of the lesson.
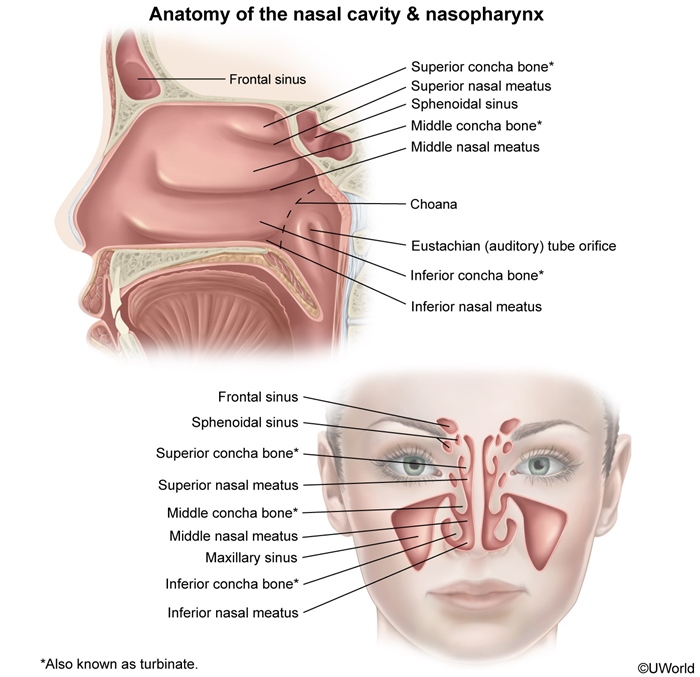
Anatomy Overview & The Common Cold
The upper respiratory tract includes the nasal cavity, paranasal sinuses, pharynx, tonsils, and larynx. Understanding the drainage of the sinuses and the Eustachian tube helps explain why one viral URI can spread to cause sinusitis or otitis media.
Common Cold (Viral Nasopharyngitis)
- Cause: rhinovirus (most common), coronavirus, RSV, parainfluenza, adenovirus.
- Features: rhinorrhea, nasal congestion, sneezing, sore throat, mild cough, low-grade fever. Lasts 7–10 days.
- Diagnosis: clinical.
- Treatment: supportive only — fluids, rest, saline drops, paracetamol for fever. No antibiotics.
- Avoid over-the-counter cough/cold medicines in children <6 years (no benefit, can cause harm).
- No aspirin in children (risk of Reye syndrome).
Refer to the distinguishing features of common upper respiratory illnesses for a quick viral URI vs influenza vs strep pharyngitis comparison.
Acute Pharyngitis & Tonsillitis
Sore throat is one of the most common pediatric complaints. The key clinical task is to separate viral pharyngitis (the majority) from Group A Streptococcus (GAS) pharyngitis, which requires antibiotics to prevent rheumatic fever.
Viral vs GAS Pharyngitis
- Viral (most common): cough, rhinorrhea, hoarseness, conjunctivitis, oral ulcers. Adenovirus, EBV, coxsackievirus.
- GAS (Streptococcus pyogenes): sudden fever, sore throat, tonsillar exudate, tender anterior cervical lymphadenopathy, palatal petechiae. No cough, no rhinorrhea. Age 5–15 years.
Diagnosis
- Centor / McIsaac criteria guide testing.
- Rapid antigen detection test (RADT) — first-line. If negative in a child, confirm with throat culture (gold standard).
Treatment of GAS pharyngitis
- First-line: Penicillin V oral 250 mg BID–TID × 10 days (or amoxicillin 50 mg/kg/day × 10 days — better taste for kids).
- One-dose option: Benzathine penicillin G IM (single dose).
- Penicillin allergy: Cephalexin, clindamycin, or azithromycin.
Treatment prevents acute rheumatic fever (if started within 9 days) but does not prevent post-streptococcal glomerulonephritis. See the streptococcal pharyngitis symptoms, diagnosis, treatment, and complications table for the full criteria and antibiotic options.
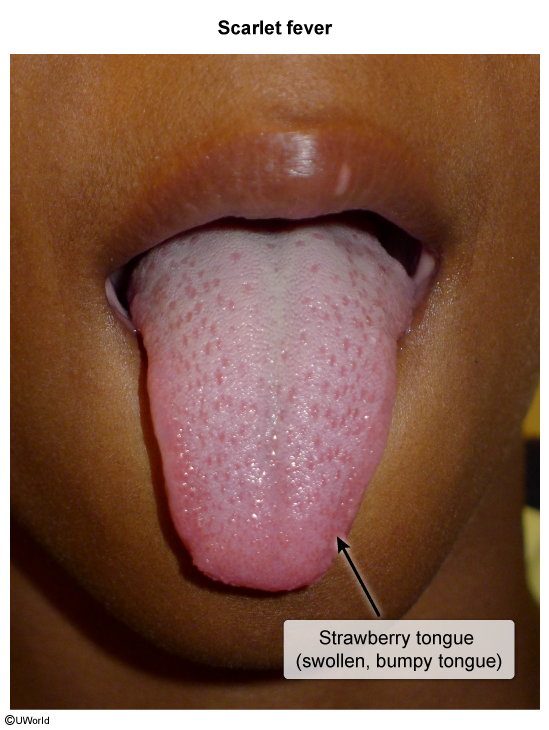
Scarlet Fever
Toxin-mediated GAS variant: strawberry tongue, fine sandpaper rash, and circumoral pallor. Same treatment (penicillin).
Infectious Mononucleosis (EBV)
- Adolescent with fever, sore throat, posterior cervical lymphadenopathy, splenomegaly, fatigue.
- Exudative tonsillitis can mimic GAS.
- Monospot test (heterophile antibodies); atypical lymphocytes on smear.
- Avoid amoxicillin / ampicillin → causes a diffuse maculopapular rash in ~90%.
- Avoid contact sports for ≥3–4 weeks (risk of splenic rupture).
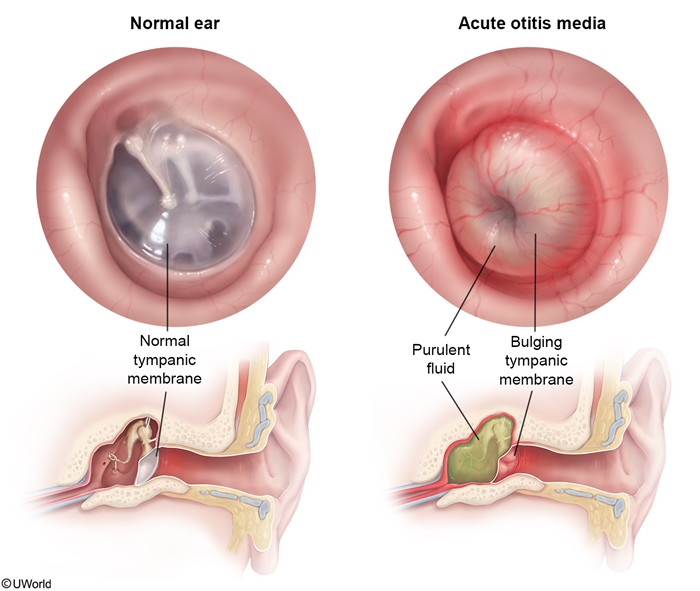
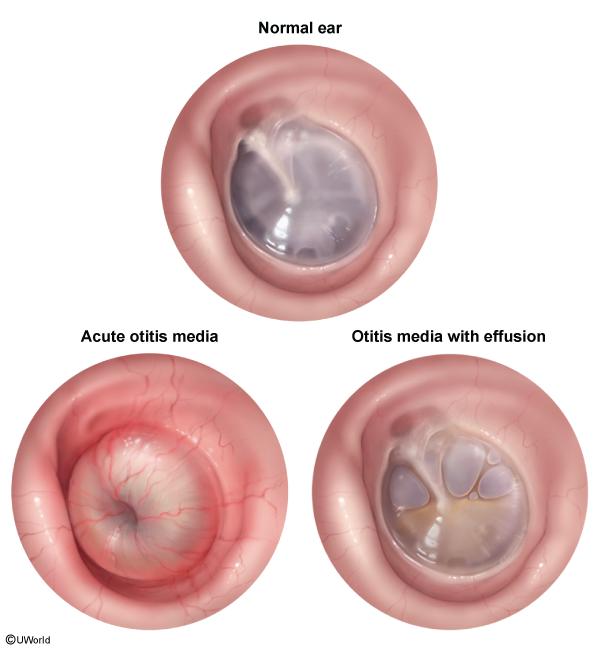
Acute Otitis Media (AOM)
Acute otitis media is the most common bacterial complication of a viral URI in children. A blocked Eustachian tube traps fluid in the middle ear, which then gets infected.
Microbiology
- Streptococcus pneumoniae (most common)
- Nontypeable Haemophilus influenzae
- Moraxella catarrhalis
Clinical Features
- Ear pain (older child), ear tugging + irritability (infant).
- Fever, decreased hearing, recent URI.
- Otoscopy (diagnostic): bulging, erythematous tympanic membrane with loss of light reflex and decreased mobility on pneumatic otoscopy.
Management
- First-line: Amoxicillin 80–90 mg/kg/day PO divided BID × 10 days.
- Second-line (or if antibiotic in last 30 days / concurrent conjunctivitis / treatment failure): Amoxicillin-clavulanate.
- Penicillin allergy: cefdinir, cefuroxime, or ceftriaxone IM (single dose).
- Observation option (no antibiotic, reassess in 48–72 hr): well-appearing child ≥2 years with mild unilateral AOM.
See the initial management of uncomplicated AOM by age and severity for the age-based observation vs antibiotic algorithm.
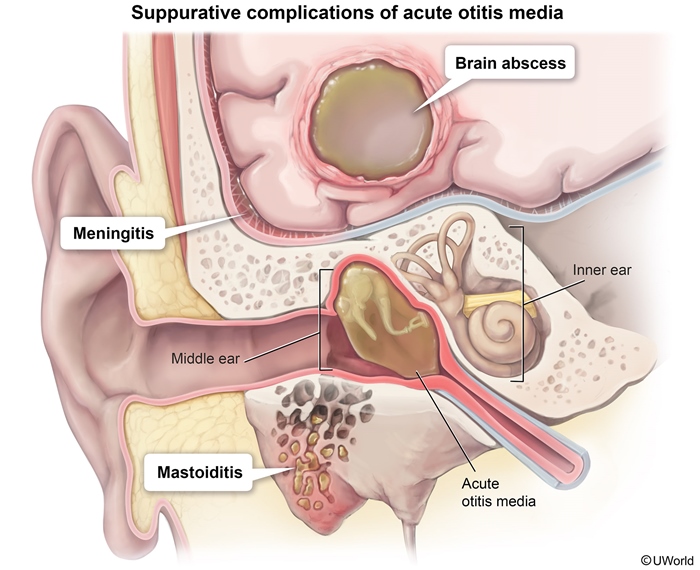
Complications
- TM perforation (sudden relief of pain + otorrhea).
- Acute mastoiditis — postauricular swelling, erythema, ear pushed forward.
- Rare: meningitis, brain abscess, cavernous sinus thrombosis.
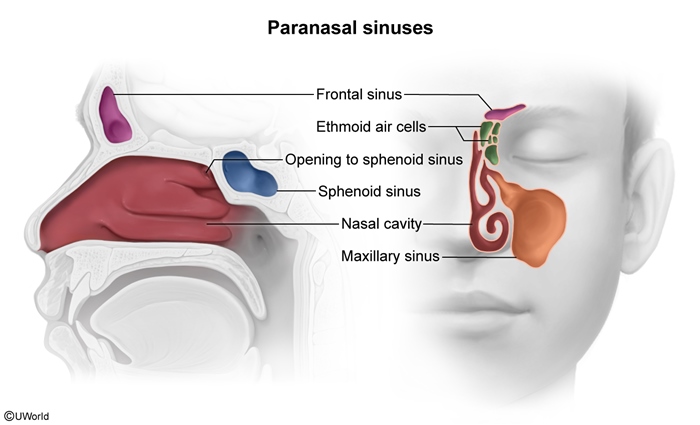
Acute Rhinosinusitis
Inflammation of the paranasal sinus mucosa. Most cases are viral and self-limited. Bacterial sinusitis is diagnosed by duration and pattern, not by colour of nasal secretions.
Acute Bacterial Rhinosinusitis (ABRS) — diagnosis
Diagnose ABRS when a URI shows one of:
- Persistent symptoms ≥10 days without improvement.
- Severe symptoms ≥3 days (high fever ≥39 °C + purulent discharge + facial pain).
- "Double sickening" — initial improvement, then worsening (biphasic course).
Pathogens
Same as AOM: S. pneumoniae, nontypeable H. influenzae, M. catarrhalis.
Treatment
- First-line: Amoxicillin-clavulanate (45–90 mg/kg/day of amoxicillin component, PO BID × 10–14 days).
- Penicillin allergy: doxycycline (adults) or levofloxacin.
- Supportive: saline irrigation, intranasal corticosteroids.
See the acute bacterial rhinosinusitis criteria and treatment for the full diagnostic thresholds and antibiotic stewardship pearls.
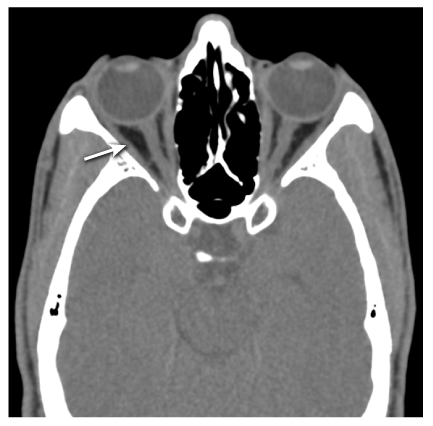
Red-flag Complications
- Periorbital / orbital cellulitis (especially from ethmoid sinus).
- Cavernous sinus thrombosis — bilateral CN III, IV, V₁, V₂, VI palsies, proptosis.
- Frontal sinusitis → Pott's puffy tumour (frontal bone osteomyelitis with forehead swelling).
- Brain abscess, meningitis.
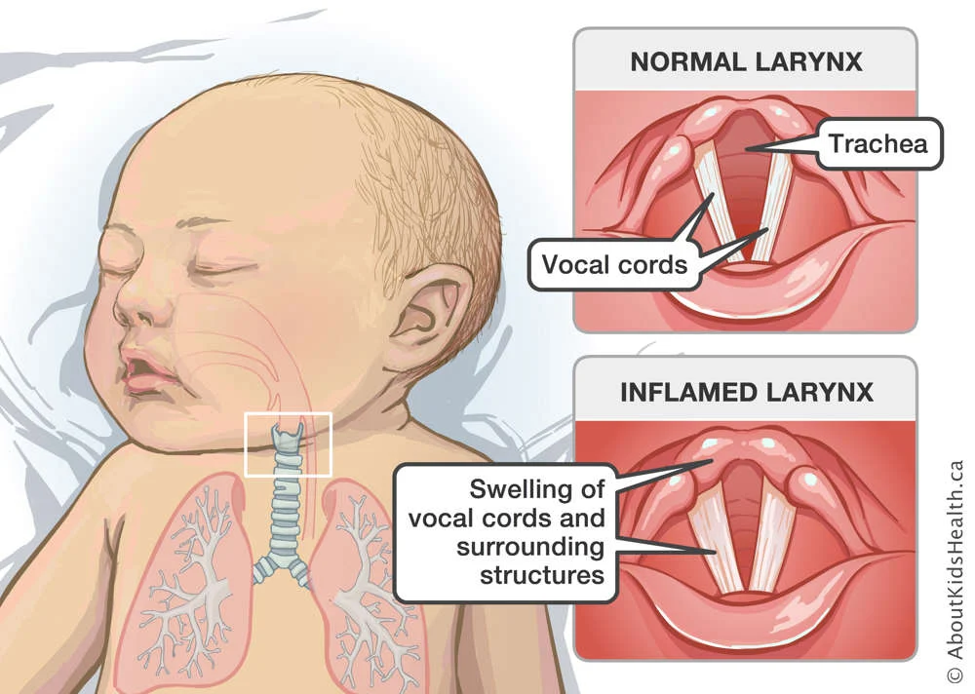
Croup (Laryngotracheobronchitis)
Croup is a viral inflammation of the larynx, trachea, and bronchi. Subglottic edema produces the classic barking cough and inspiratory stridor.
Epidemiology
- Age: 6 months – 3 years (peak ~2 years).
- Season: autumn and early winter.
Etiology
- Parainfluenza virus types 1 and 2 (most common).
- Others: parainfluenza 3, influenza, RSV, adenovirus, measles.
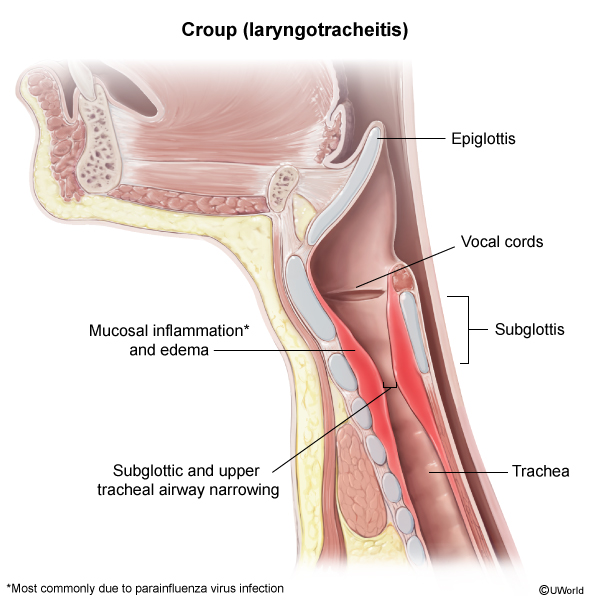
Clinical Features
- Low-grade fever and URI symptoms for 1–2 days, then:
- Barking ("seal-like") cough
- Inspiratory stridor
- Hoarseness
- Symptoms worse at night and when the child is agitated.
- Child is not toxic-appearing.
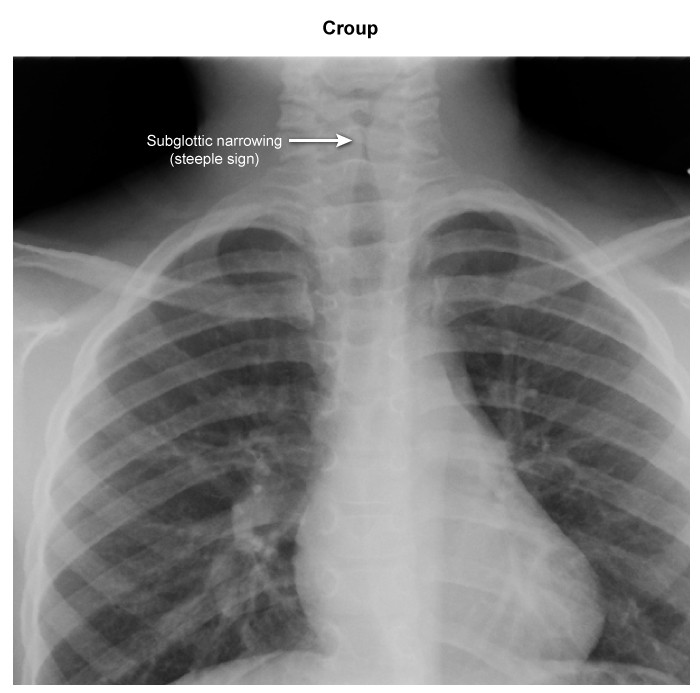
Diagnosis
Clinical diagnosis. Imaging is not routinely required.
If done, AP neck X-ray shows the "steeple sign" — subglottic narrowing of the trachea.
Management
- Mild (no stridor at rest, no retractions): Single dose dexamethasone 0.6 mg/kg PO/IM/IV (max 10 mg). Cool mist / humidified air at home.
- Moderate to severe (stridor at rest, retractions): Dexamethasone + nebulized epinephrine (racemic or L-epinephrine).
- Observe in the ED for 3–4 hours after epinephrine — risk of rebound stridor as the drug wears off (~2 hours).
- Hospitalize if the child needs >2 doses of nebulized epinephrine or has persistent stridor at rest.
Spasmodic Croup
A non-infectious variant. Child wakes suddenly at night with barking cough and stridor, then is asymptomatic by morning. May recur over 2–3 nights. No fever. Recurrent episodes may indicate a variant of asthma.
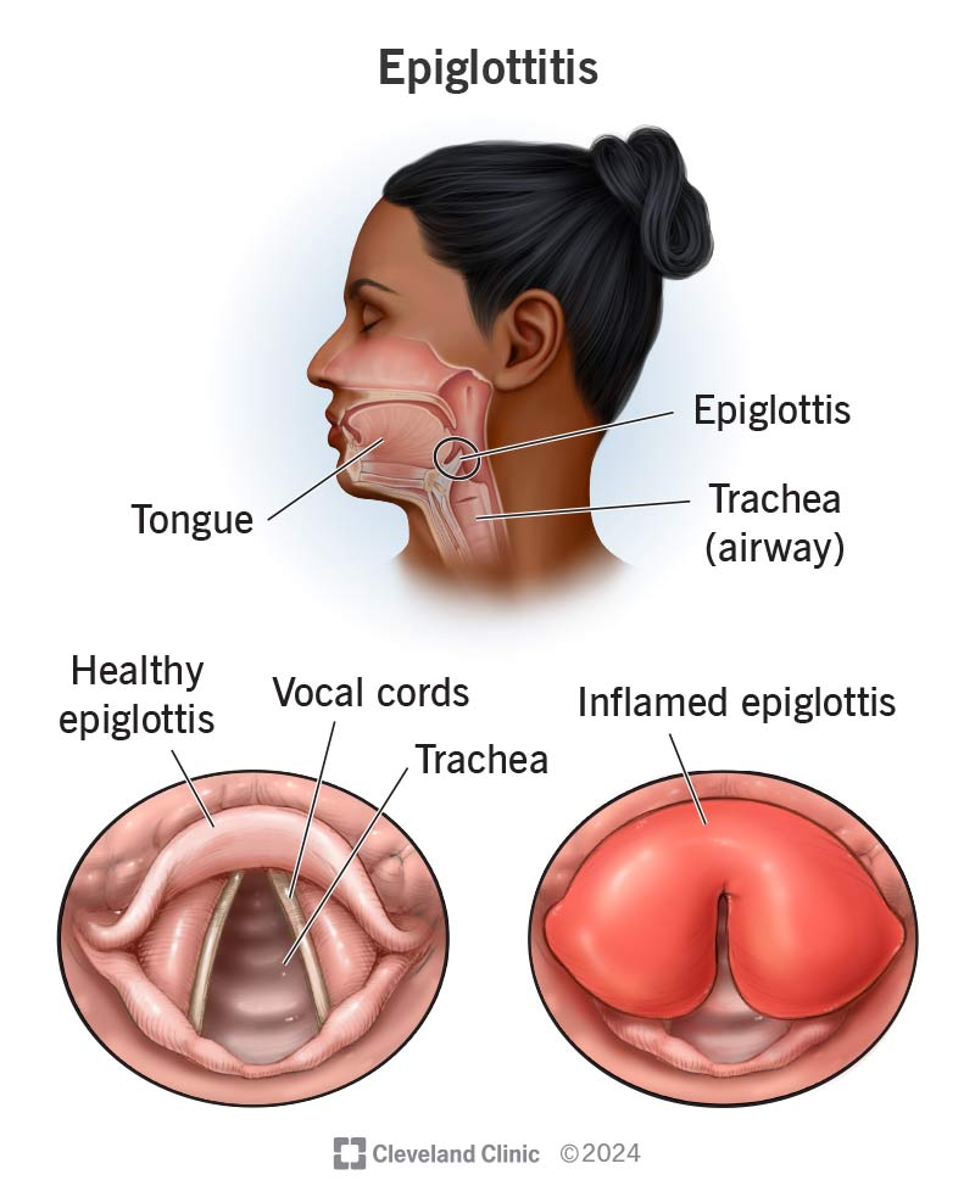
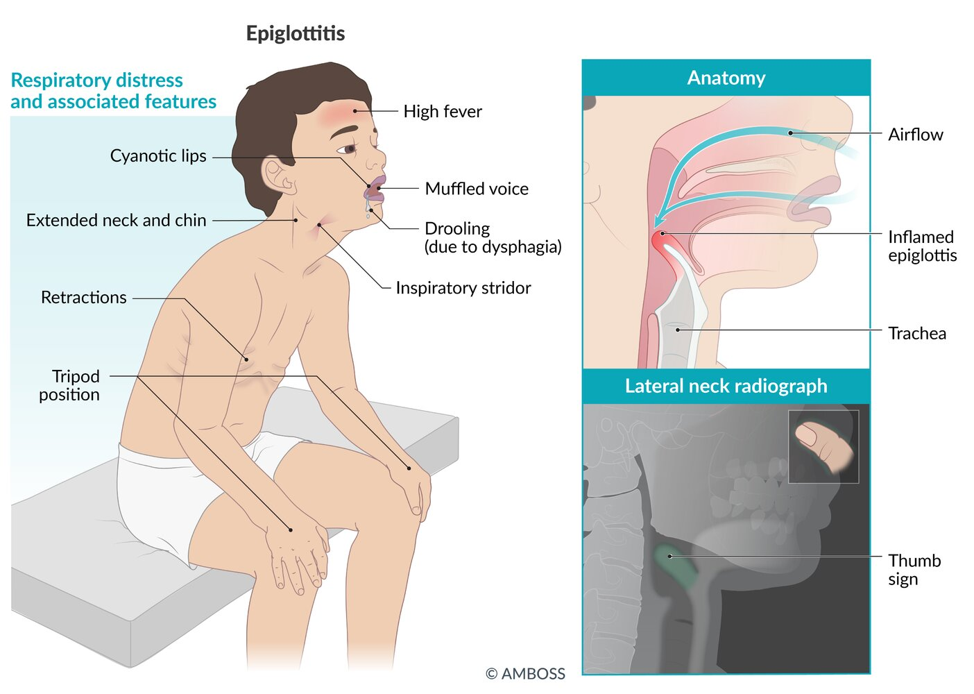
Epiglottitis
A life-threatening pediatric airway emergency: rapid swelling of the epiglottis can completely obstruct the airway within hours.
Epidemiology & Etiology
- Age: classically 2–5 years (any age possible).
- Now rare because of the Hib vaccine.
- Classic cause: Haemophilus influenzae type b (Hib) — still important in unvaccinated children.
- In vaccinated populations: nontypeable H. influenzae, S. pneumoniae, S. pyogenes, S. aureus.
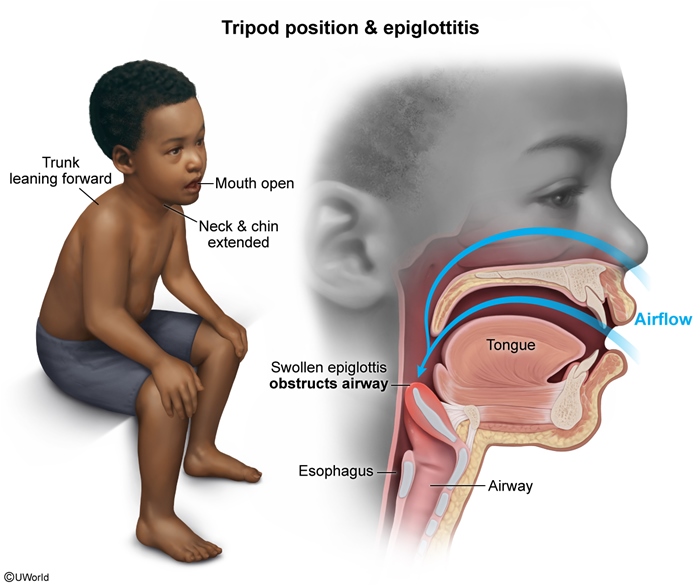
Clinical Features — the "4 D's"
- Dysphagia (difficulty swallowing)
- Drooling
- Dysphonia (muffled "hot potato" voice)
- Distress — tripod / sniffing position, inspiratory stridor
Plus abrupt onset, high fever, sore throat, and a toxic-appearing child. No barking cough (differentiates from croup).
Diagnosis
- Clinical diagnosis — do NOT delay airway management for tests.
- Lateral neck X-ray (if stable): "thumb sign" — swollen epiglottis.
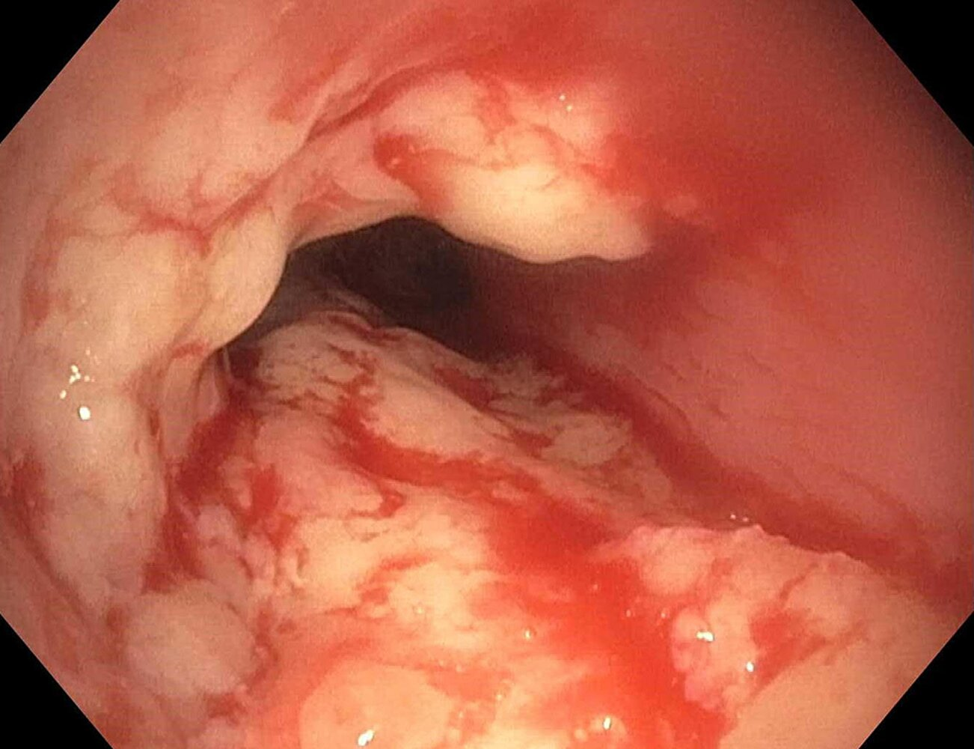
- Gold standard: direct visualization of a cherry-red, swollen epiglottis on laryngoscopy in the operating room by an anaesthesiologist or ENT.

Management — Airway First
- Step 1: Keep the child calm and in a position of comfort (usually on parent's lap). Give blow-by oxygen. Do NOT examine the throat with a tongue depressor or perform painful procedures — can trigger laryngospasm and total obstruction.
- Step 2: Call anaesthesia and ENT immediately. Transfer to the OR for controlled endotracheal intubation (have tracheostomy backup).
- Step 3: Once airway is secured, start IV antibiotics: ceftriaxone 50 mg/kg IV daily + vancomycin (cover MRSA) for 7–10 days. Most children are bacteremic.
Prophylaxis (Hib epiglottitis)
- Rifampin for unvaccinated household contacts <4 years old (eradicates Hib carriage in 95%).
- Routine Hib immunization is the main prevention.
See the infectious epiglottitis epidemiology, clinical features, diagnosis, and treatment table for the full reference.
Bacterial Tracheitis
A bacterial superinfection of the trachea, usually following a viral URI such as croup. Because of the Hib vaccine, bacterial tracheitis is now more common than epiglottitis.
Epidemiology & Etiology
- Age: typically <3 years.
- Season: autumn/winter, coinciding with viral epidemics.
- Most common cause: Staphylococcus aureus.
- Others: S. pneumoniae, M. catarrhalis, nontypeable H. influenzae, anaerobes.
- Usually preceded by croup (parainfluenza types 1 and 2). The epiglottis is not involved.
Clinical Features
- Child with preceding viral URI / croup who suddenly deteriorates.
- High fever, toxic-appearing.
- Brassy, productive cough with purulent secretions.
- Stridor that does NOT respond to dexamethasone or nebulized epinephrine — this is the key clue.
- No drooling, no dysphagia (helps differentiate from epiglottitis).
Diagnosis
- Clinical + bronchoscopy: thick purulent tracheal secretions and pseudomembranes. Bronchoscopy is both diagnostic and therapeutic (suction).
- Neck X-ray may show subglottic narrowing with a ragged/irregular tracheal mucosa.
- Culture of tracheal secretions to guide antibiotics.
Management
- Step 1: Airway support — intubation or tracheostomy is frequently required due to thick secretions and obstruction.
- Step 2: Empiric IV antibiotics covering S. aureus: nafcillin/oxacillin (MSSA) or vancomycin (if MRSA common locally), plus ceftriaxone for gram-negatives.
- Step 3: Continue for 10–14 days; most children improve clinically within 2–3 days but require prolonged hospitalization due to airway edema.
Comparison: Croup vs Epiglottitis vs Bacterial Tracheitis
The three classic "stridor + fever" pediatric emergencies are differentiated by onset speed, toxicity, cough character, and X-ray sign. This is one of the highest-yield pediatric tables for the SMLE/internship exam.
| Croup vs Epiglottitis vs Bacterial Tracheitis | |||
|---|---|---|---|
| Feature | Croup | Epiglottitis | Bacterial Tracheitis |
| Age | 6 mo–3 yr | 2–5 yr | <3 yr |
| Cause | Parainfluenza virus (types 1, 2) | Hib (classic); now nontypeable H. influenzae, S. pneumoniae, S. aureus | S. aureus (after viral URI) |
| Onset | Gradual, worse at night | Abrupt, toxic-appearing | Viral URI → sudden deterioration |
| Fever | Low-grade | High | High |
| Cough | Barking ('seal-like') | Usually absent | Brassy, productive |
| Stridor | Inspiratory | Inspiratory, muffled voice | Inspiratory (does not respond to croup Tx) |
| Position | Comfortable | Tripod, sniffing, drooling | Variable, toxic |
| X-ray | Steeple sign (AP neck) | Thumb sign (lateral neck) | Subglottic narrowing + irregular tracheal wall |
| Treatment | Dexamethasone ± nebulized epinephrine | Secure airway + ceftriaxone + vancomycin | Intubation often needed + nafcillin/vancomycin |
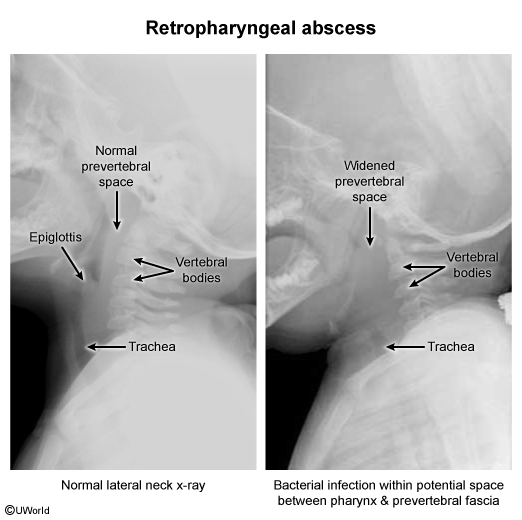
Also remember a fourth important differential of stridor in children — retropharyngeal abscess — which shows widened prevertebral soft tissue on lateral neck X-ray, with neck stiffness and dysphagia.
Mnemonics
| Mnemonics – جمل تذكرية | |
Epiglottitis — the 4 D's: Croup vs Epiglottitis X-ray: GAS pharyngitis = Centor criteria (CENTOR): AOM & sinusitis bugs — "Some Have Middle-ear infections": Mononucleosis triad — "Fever, Pharyngitis, Lymphadenopathy" + splenomegaly. Avoid amoxicillin → rash. |
جملة تذكرية |
Key Points for Exams
- Most URTIs are viral → supportive care only. No antibiotics for the common cold.
- Avoid OTC cough/cold medications in children <6 years.
- GAS pharyngitis → diagnose with rapid strep test, confirm negatives with throat culture. Treat with penicillin V × 10 days (or amoxicillin) to prevent rheumatic fever.
- Adolescent with sore throat + amoxicillin → maculopapular rash = EBV mononucleosis, not penicillin allergy.
- AOM first-line: high-dose amoxicillin 80–90 mg/kg/day. Switch to amoxicillin-clavulanate if treatment failure, recent antibiotics, or AOM with conjunctivitis.
- Acute bacterial sinusitis criteria: ≥10 days persistent OR severe ≥3 days OR biphasic worsening → amoxicillin-clavulanate.
- Croup = barking cough + inspiratory stridor + low fever + steeple sign. Treat with dexamethasone (all cases) ± nebulized epinephrine (stridor at rest). Observe ≥3–4 hr after epinephrine for rebound.
- Epiglottitis = abrupt high fever + drooling + tripod + no cough + thumb sign. Do NOT examine throat. Secure airway in OR, then ceftriaxone + vancomycin.
- Bacterial tracheitis = a child with croup who fails to respond to dexamethasone and epinephrine, gets toxic, and has a brassy productive cough. Cause: S. aureus. Treat with intubation + nafcillin/vancomycin.
- X-ray signs to memorize:
- Croup → Steeple sign (AP neck)
- Epiglottitis → Thumb sign (lateral neck)
- Retropharyngeal abscess → Widened prevertebral space (lateral neck)
- Hib vaccine dramatically reduced epiglottitis; bacterial tracheitis is now more common than epiglottitis.
- Mastoiditis = most common suppurative complication of AOM → postauricular swelling, ear pushed forward. IV antibiotics + ENT referral for possible mastoidectomy.
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.