Summary
- Pertussis (whooping cough) = highly contagious respiratory infection caused by Bordetella pertussis, a gram-negative coccobacillus.
- Spreads via respiratory droplets; most severe in infants < 6 months.
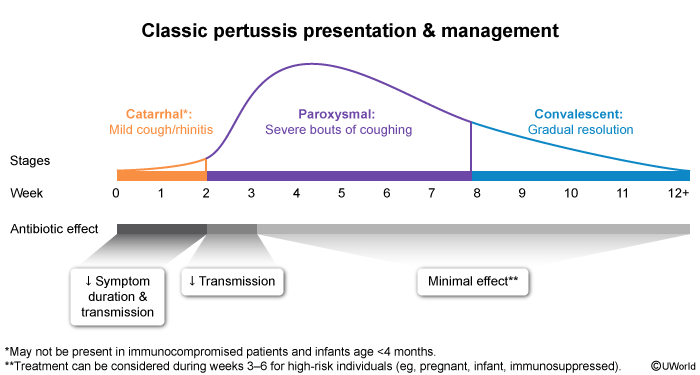
- Three clinical phases: catarrhal (cold-like, 1–2 weeks) → paroxysmal (whooping cough + posttussive vomiting, 2–6 weeks) → convalescent (gradual recovery, weeks to months).
- Diagnosis: nasopharyngeal PCR (best) or culture; CBC shows lymphocyte-predominant leukocytosis.
- Treatment: macrolides (azithromycin first line). Trimethoprim–sulfamethoxazole (TMP-SMX) if macrolide-allergic.
- Prevention: DTaP in children, Tdap booster in adolescents/adults and every pregnancy.
Etiology and Microbiology
- Bordetella pertussis — main pathogen; gram-negative, aerobic coccobacillus.
- Bordetella parapertussis — causes a milder, clinically similar illness.
- Humans are the only reservoir; transmission is via respiratory droplets.
Epidemiology
- Highest risk: infants < 6 months (immune system immature, primary DTaP series incomplete).
- Main source of infection for children = adolescents and adults with waning immunity (often present with prolonged cough).
- Routine immunization beginning at 2 months has greatly reduced incidence, but outbreaks still occur in under-vaccinated communities.
- Incubation period: 7–10 days (range up to 3 weeks).
Pathophysiology
- Bacteria attach to ciliated respiratory epithelium via adhesins (e.g., filamentous hemagglutinin, pertactin).
- Release of pertussis toxin (PT) is the key virulence step:
- PT ADP-ribosylates the Gi protein → inactivates inhibition of adenylate cyclase → ↑ intracellular cAMP.
- Result: lymphocytosis (impaired lymphocyte trafficking into tissues) and impaired phagocyte function.
- Tracheal cytotoxin damages ciliated cells → impaired mucus clearance → severe paroxysmal cough.
| Mnemonic — Pertussis toxin | |
"Pertussis is Inhibited Gi" → Pertussis toxin ADP-ribosylates Gi, disabling its inhibitory action on adenylate cyclase → ↑ cAMP → lymphocytosis and impaired phagocyte function. (Cholera = Gs ↑; Pertussis = Gi block — both raise cAMP.) |
جملة تذكرية |
The bacterial-toxin mechanism is summarised in detail in the Mechanisms of Action of Bacterial Toxins reference.
Clinical Features
Pertussis classically progresses through 3 stages:
1. Catarrhal stage (1–2 weeks)
- Looks like a common cold: rhinorrhea, nasal congestion, mild conjunctival redness, low-grade fever, mild cough.
- Most contagious phase — diagnosis is rarely made here.
2. Paroxysmal stage (1–6 weeks)
- Paroxysms of coughing — the hallmark of pertussis.
- Coughing fits often end with an inspiratory "whoop" (more common in older children/adults than in infants).
- Post-tussive vomiting is characteristic.
- Between attacks the child looks well and is afebrile.
- Young infants may present with apnea, cyanosis, or choking — sometimes without a true whoop.
3. Convalescent stage (weeks to months)
- Cough gradually becomes less frequent and less severe.
- Duration: 6–10 weeks in children; many adolescents/adults cough > 10 weeks ("100-day cough").
Diagnosis
Diagnosis is mainly clinical, then confirmed in the lab.
- Clinical clue: cough lasting ≥ 2 weeks + paroxysms, inspiratory whoop, OR post-tussive vomiting.
- Blood: CBC with marked lymphocyte-predominant leukocytosis (a key clue, especially in infants).
- Nasopharyngeal swab — first-line confirmatory test:
- PCR — best sensitivity, preferred test in the first 3–4 weeks of cough.
- Culture on Bordet-Gengou or Regan-Lowe media — highly specific but slow and less sensitive after the first 2 weeks.
- Serology — useful only late (after 3–4 weeks of cough) when PCR/culture are negative.
- Chest X-ray — usually normal; may show perihilar infiltrates ("shaggy right heart border") or rule out pneumonia.
| Important – فكرة سؤال | |
A young infant presenting with apnea, cyanosis, or post-tussive vomiting — even without a classic "whoop" — should raise immediate suspicion for pertussis. Infants < 6 months may never develop the whoop because they lack the inspiratory force. |
تذكر |
See the CDC diagnostic criteria for Bordetella pertussis for the full probable-vs-confirmed case definition.
Management
Supportive care
- Hospitalize infants < 6 months (or any patient with apnea, cyanosis, severe paroxysms, feeding difficulty, or pneumonia).
- Provide oxygen, hydration, and nutritional support; suction secretions gently.
- Droplet precautions until the patient has received at least 5 days of effective antibiotics.
Antibiotics — macrolides are first line
- Azithromycin — drug of choice (all ages, including < 1 month).
- Infants < 6 months: 10 mg/kg PO once daily × 5 days.
- Children ≥ 6 months: 10 mg/kg (max 500 mg) day 1, then 5 mg/kg (max 250 mg) once daily × 4 days.
- Adults: 500 mg PO day 1, then 250 mg once daily × 4 days.
- Clarithromycin — 7-day course; only for ≥ 1 month of age.
- Erythromycin — 14-day course; avoid in infants < 1 month (linked to infantile hypertrophic pyloric stenosis).
- Macrolide-allergic patients → TMP-SMX (only in children ≥ 2 months).
Key timing point
- Antibiotics shorten the disease only if started in the catarrhal phase or very early paroxysmal phase.
- If given later, they do not change the patient's course — but they reduce transmission, which is why they are still indicated.
Vaccine update
- Give any due booster doses (DTaP in children; Tdap in adolescents 11–18 years and unvaccinated adults).
Postexposure Prophylaxis
Give PEP regardless of vaccination status, started as soon as possible (ideally within 21 days of exposure).
Indications
- Close contacts of a symptomatic patient (household members, direct contact with respiratory secretions).
- High-risk contacts even with limited exposure:
- Pregnant women (especially third trimester).
- Infants and young children.
- Immunocompromised individuals.
Regimen (same drugs as treatment)
- Age < 1 month: Azithromycin only.
- Age ≥ 1 month: Azithromycin, clarithromycin, or erythromycin.
- If macrolide-allergic and ≥ 2 months: TMP-SMX.
| Note – ملاحظة | |
Erythromycin in neonates < 1 month is associated with infantile hypertrophic pyloric stenosis. For this age group, azithromycin is the macrolide of choice. |
ملاحظة |
Refer to the pertussis postexposure prophylaxis indications and treatment table for the full age-stratified regimens.
Prevention and Vaccination
DTaP (pediatric)
- Acellular pertussis component combined with diphtheria and tetanus toxoids.
- 5-dose schedule: 2, 4, 6 months; 15–18 months; 4–6 years.
- Absolute contraindications:
- Anaphylaxis to a previous dose or vaccine component.
- Encephalopathy within 7 days of a prior dose (with no other cause identified).
Tdap (adolescent/adult booster)
- One dose at age 11–12 years, then a Td or Tdap booster every 10 years.
- Pregnancy: give Tdap in every pregnancy between 27–36 weeks gestation — produces maternal antibodies that protect the newborn until DTaP can be started.
- Cocooning: vaccinate all close contacts of newborns (parents, grandparents, caregivers) to reduce transmission.
See the DTaP immunization schedule and contraindications and the Tdap administration during pregnancy references for full details.
Complications
Highest-risk patients
- Infants < 6 months.
- Preterm infants.
- Unimmunized or under-immunized infants.
Major complications
- Apnea and cyanosis (often the presenting feature in young infants).
- Secondary bacterial pneumonia — the most common cause of death.
- Seizures and pertussis encephalopathy (from hypoxia).
- Mechanical complications of forceful coughing: subconjunctival hemorrhage, rib fractures, urinary incontinence, hernia.
- Death — almost entirely in young, unvaccinated infants.
Key Points for Exams
| Key Points for Exams – نقاط مهمة للامتحانات | |
|
تذكر |
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.