Summary
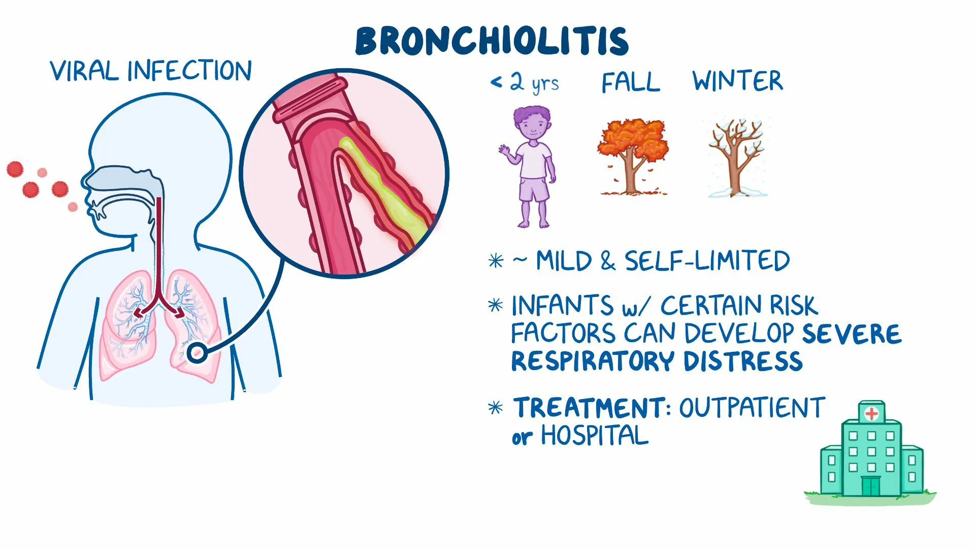
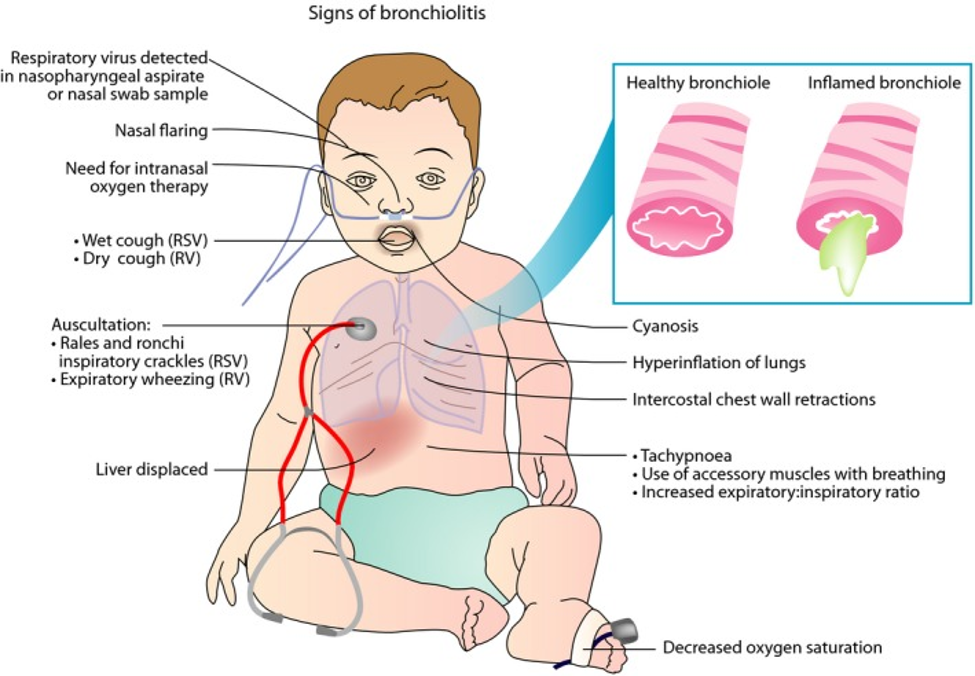
Acute bronchiolitis is an inflammatory obstruction of the small airways (bronchioles) caused by a viral lower respiratory tract infection, most often respiratory syncytial virus (RSV). It is the most common lower respiratory infection in infants under 2 years.
The typical patient is an infant who starts with a runny nose and cough, then over a few days develops wheezing, crackles, tachypnea, and retractions. Diagnosis is clinical. Treatment is supportive only — nasal suctioning, hydration, and oxygen when needed. Most cases recover; the main danger is apnea in very young infants and respiratory failure in high-risk babies.
| Acute Bronchiolitis — At a Glance | |
| Basics | Definition & cause |
| Age | < 2 years (peak 2–6 months) |
| Cause | RSV (most common); also parainfluenza, hMPV, rhinovirus |
| Season | Winter – early spring |
| Clinical | Diagnosis & treatment |
| Hallmark | URI prodrome → wheezing + crackles + respiratory distress |
| Diagnosis | Clinical (CXR/viral testing not routine) |
| Treatment | Supportive: suctioning, hydration, O₂ if SpO₂ < 90% |
| Outcomes | Prevention & complications |
| Prevention | Palivizumab / nirsevimab in high-risk infants |
| Key complication | Apnea (especially infants < 2 months) |
Epidemiology and Risk Factors
- Most common lower respiratory infection in the first 2 years of life.
- Most common cause of hospitalization during the first year.
- Almost all children get RSV by age 2 — but only some develop bronchiolitis.
- Season: November to April (winter–early spring).
- Sex: Males > females (≈ 2 : 1).
Risk factors for getting bronchiolitis
- Daycare attendance.
- Second-hand smoke exposure.
- Family history of asthma or atopy.
- Crowded living conditions.
- Lack of breastfeeding.
- Low birth weight.
Risk factors for severe disease (need hospitalization / ICU)
- Age < 3 months (especially < 2 months — apnea risk).
- History of prematurity.
- Chronic lung disease of prematurity (BPD).
- Hemodynamically significant congenital heart disease.
- Immunodeficiency.
- Genetic / neuromuscular abnormalities.
Etiology
Acute bronchiolitis is almost always viral. The leading pathogen by far is:
- Respiratory syncytial virus (RSV) — causes the majority of cases. RSV is an enveloped, negative-sense, single-stranded RNA virus in the Pneumoviridae family (previously classified with Paramyxoviridae).
Other less common causes:
- Parainfluenza virus
- Human metapneumovirus (hMPV)
- Influenza virus
- Rhinovirus
- Coronavirus
- Human bocavirus
- Adenovirus (can cause severe disease)
| Mnemonic – جملة تذكرية | |
|
RSV = Respiratory Syncytial Virus → "Runs through nurseries in Snow season, causes Viral wheeze." |
جملة تذكرية |
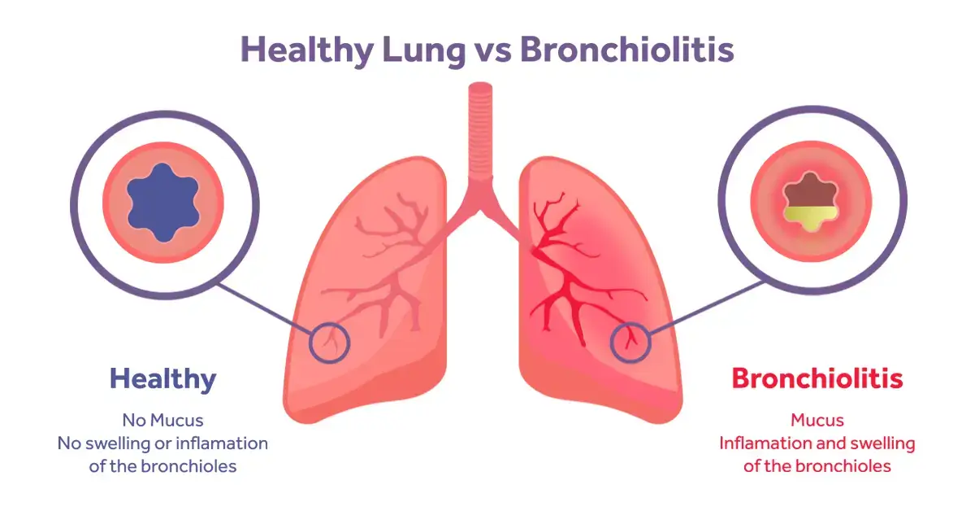
Pathophysiology
The virus infects and damages the ciliated epithelial cells of the small airways (bronchioles). This triggers a chain of events that obstructs airflow:
- Epithelial necrosis and shedding of dead cells into the airway lumen.
- Mucus hypersecretion and impaired ciliary clearance.
- Submucosal edema and peribronchial inflammation (lymphocyte infiltrate).
- The lumen fills with mucus plugs + cellular debris → partial or complete obstruction.
Because infant airways are tiny, even mild edema causes big airway narrowing. The obstruction acts as a ball-valve: air gets in during inspiration but cannot fully exit during expiration → air trapping → hyperinflation → V/Q mismatch → hypoxemia.
Clinical Features
The illness follows a typical timeline over about 7–10 days, with symptoms peaking around day 5.
Stage 1 — URI prodrome (days 1–3)
- Low-grade fever
- Runny nose / nasal congestion
- Cough
- Poor feeding
Stage 2 — Lower respiratory involvement (days 3–7)
- Tachypnea (often the earliest red flag)
- Wheezing (expiratory)
- Fine crackles (rales)
- Prolonged expiratory phase
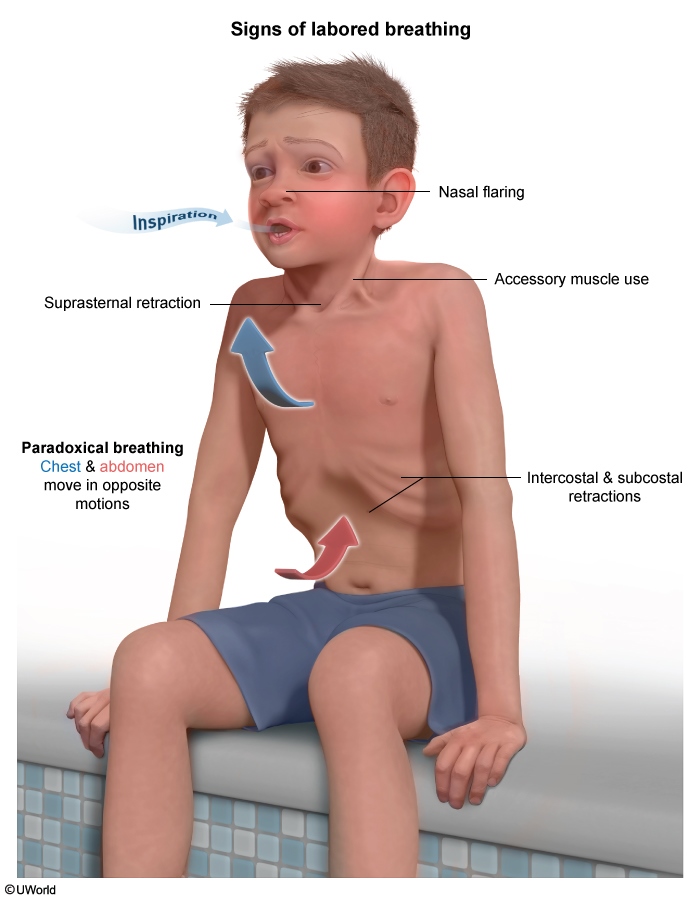
- Increased work of breathing: nasal flaring, intercostal/subcostal retractions, grunting, accessory muscle use
- Hypoxia (low SpO₂)
- Apnea — may be the first sign in infants < 2 months
| Important – فكرة سؤال | |
|
In a previously healthy infant under 2 months presenting with bronchiolitis, apnea may be the first and only sign — even before wheezing or hypoxia appears. Always admit infants < 2 months for observation. |
تذكر |
Most infants are infectious for ≈ 7 days, but some shed virus for 3–4 weeks or longer.
Diagnosis
Bronchiolitis is a clinical diagnosis. Routine labs and imaging are not needed in a typical case.
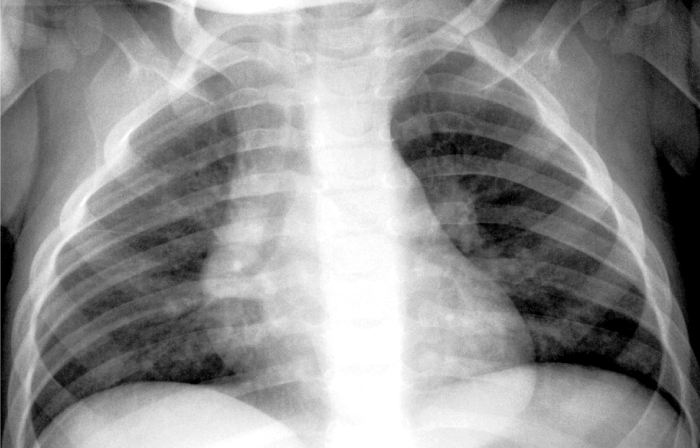
Chest X-ray (only if severe disease, atypical features, or another diagnosis suspected): nonspecific findings that include —
- Hyperinflation with air trapping (flattened diaphragms, > 6 anterior / > 10 posterior ribs visible)
- Peribronchial cuffing (haziness around bronchial walls)
- Increased interstitial markings
- Patchy atelectasis
- No focal lobar consolidation (helps rule out bacterial pneumonia)

Viral testing: Rapid immunofluorescence or enzyme immunoassays for RSV antigen in nasopharyngeal specimens are available and reliable, but routine viral identification does not change management and is not recommended in mild outpatient cases. Use it mainly for hospitalized infants for cohorting / infection control.
Refer to the Bronchiolitis reference summary for a consolidated view of pathophysiology, radiographic findings, treatment, complications, and prevention.
Differential Diagnosis
The "wheezy infant" differential is short — but each alternative has a distinguishing feature you must know.
- Asthma / viral-induced wheeze — older child, recurrent episodes, responsive to bronchodilators, family or personal atopy.
- Pneumonia — focal crackles, lobar consolidation on CXR, higher fever, looks more "toxic".
- Croup (laryngotracheitis) — stridor (not wheeze), barking cough, hoarseness, steeple sign on neck X-ray.
- Foreign body aspiration — sudden onset in a previously well toddler, focal monophonic wheeze, decreased air entry on one side.
- Heart failure — known CHD, hepatomegaly, gallop, cardiomegaly on CXR.
- Pertussis — paroxysmal cough, inspiratory whoop, post-tussive vomiting, lymphocytosis.
| Bronchiolitis vs Croup vs Pneumonia (quick differential) | |||
|---|---|---|---|
| Feature | Bronchiolitis | Croup | Pneumonia |
| Age | < 2 years | 6 mo – 6 yrs | Any |
| Cause | RSV | Parainfluenza | Bacterial / viral |
| Sound | Wheeze + crackles | Stridor + barking cough | Crackles, ↓ breath sounds |
| CXR | Hyperinflation, peribronchial cuffing | Steeple sign (neck X-ray) | Lobar consolidation |
| Treatment | Supportive | Dexamethasone ± nebulized epinephrine | Antibiotics if bacterial |
See the Key respiratory tract infections in children for the full side-by-side comparison of nasopharyngitis, croup, bronchiolitis, pertussis, and epiglottitis.
Management
Treatment is supportive. There is no antiviral cure for routine RSV bronchiolitis.
Outpatient (mild disease)
- Nasal bulb suctioning — especially before feeds and sleep (infants are obligate nose-breathers).
- Maintain hydration — small frequent feeds.
- Antipyretics for fever.
- Educate parents on red flags: worsening retractions, refusing feeds, lethargy, cyanosis, apnea.
Indications for hospitalization
- SpO₂ < 90% on room air / persistent hypoxemia
- Significant respiratory distress (marked retractions, RR > 70)
- Inability to feed / dehydration
- Apnea
- Toxic appearance
- Age < 2–3 months
- High-risk comorbidity (BPD, CHD, immunodeficiency)
- Unreliable caregiver or social concerns
Inpatient care (stepwise)
- Step 1 — Oxygen: Supplemental O₂ to keep SpO₂ ≥ 90%. Start with nasal cannula.
- Step 2 — Hydration: NG or IV fluids if unable to feed by mouth.
- Step 3 — Nasal suctioning as needed; minimal handling.
- Step 4 — Escalate respiratory support if worsening: high-flow nasal cannula → CPAP → intubation + mechanical ventilation.
- Step 5 — Consider inhaled hypertonic saline (3%) as a mucolytic in hospitalized infants (optional, not in outpatient setting).
Therapies that are NOT recommended routinely
- Albuterol / bronchodilators — not recommended for first-time wheezing in bronchiolitis. (May trial in older infants with personal/family atopy and continue only if clear response.)
- Corticosteroids — no benefit.
- Antibiotics — not indicated unless documented bacterial co-infection (e.g., otitis media, bacterial pneumonia).
- Chest physiotherapy — no benefit.
- Ribavirin — reserved for critically ill or immunocompromised children only.
| Note – ملاحظة | |
Hospitalized RSV patients require contact precautions (gown + gloves, dedicated equipment) to prevent nosocomial spread. RSV survives hours on surfaces and is a major cause of inpatient outbreaks. |
ملاحظة |
Prevention — RSV Immunoprophylaxis
Natural RSV infection does not give lasting immunity — reinfection throughout life is common. Prevention focuses on passive immunoprophylaxis for high-risk infants during the RSV season.
Agents
- Palivizumab — monoclonal antibody against RSV F protein. Dose: 15 mg/kg IM monthly, up to 5 doses during RSV season.
- Nirsevimab — newer long-acting monoclonal antibody; a single IM dose covers an entire RSV season. Increasingly used as first-line where available.
Who qualifies (high-risk infants)
- Infants born at < 29 weeks gestation, in their 1st RSV season (age < 12 months at season start).
- Infants < 24 months with chronic lung disease of prematurity requiring medical therapy within 6 months of RSV season start.
- Infants < 24 months with hemodynamically significant congenital heart disease (cyanotic or acyanotic).
- Infants who are immunocompromised or have significant pulmonary / neuromuscular disease impairing airway clearance.
Discontinue prophylaxis for the remainder of the season if the infant is hospitalized with breakthrough RSV infection.
| Note – ملاحظة | |
Chronic lung disease of prematurity (BPD) is defined as needing supplemental oxygen for > 28 days in infants born at < 32 weeks of gestation. This is a key qualifying condition for RSV immunoprophylaxis. |
ملاحظة |
General prevention measures
- Hand hygiene (single most effective measure).
- Avoid second-hand smoke.
- Encourage breastfeeding.
- Avoid crowded daycare in high-risk infants during peak season.
Complications and Prognosis
Complications
- Apnea — especially infants < 2 months and ex-premature infants.
- Respiratory failure — may require CPAP or intubation.
- Dehydration from poor feeding.
- Bacterial superinfection — otitis media is the most common; bacterial pneumonia is uncommon but possible.
- Death — rare in previously healthy infants; risk is concentrated in those with prematurity, BPD, or significant CHD.
Prognosis
- Most healthy infants recover fully within 1–2 weeks. Cough may linger for 3–4 weeks.
- Recurrent wheezing episodes for months to years after a severe episode are common (especially after RSV).
- Association with later development of asthma is recognized but causality is debated.
Key Points for Exams – نقاط مهمة للامتحانات
- Definition: Viral inflammation of bronchioles in children < 2 years.
- #1 cause: RSV — negative-sense ssRNA virus, winter–spring epidemics.
- Classic stem: Infant with a few days of runny nose → now wheezing, crackles, tachypnea, retractions.
- Diagnosis: Clinical. CXR and viral testing are not routine.
- CXR (if done): hyperinflation + peribronchial cuffing, no focal consolidation.
- Treatment: Supportive only — suctioning, hydration, O₂ to keep SpO₂ ≥ 90%.
- Do NOT give routinely: antibiotics, corticosteroids, bronchodilators, chest physiotherapy.
- Ribavirin → only in critically ill or immunocompromised.
- Apnea is the dreaded complication in infants < 2 months — admit and monitor.
- Prevention: Palivizumab (monthly × 5) or nirsevimab (single dose) for high-risk infants: prematurity < 29 wks, BPD, significant CHD, immunocompromised.
- Isolation: hospitalized RSV → contact precautions.
- Differential trap: Stridor + barking cough = croup, not bronchiolitis. Sudden monophonic wheeze in a toddler = think foreign body.
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.