Introduction
- Nutritional Disorders are a group of disorders that refer to clinical syndromes resulting from abnormal nutrition.
- There are several indicators used to assess the nutritional status, including; weight-for-age, height-for-age, weight for height.
- Weight for age is the most commonly used parameter for nutritional status
| Indicator | Definition | Clinical Interpretation |
| Wasting |
|
|
| Stunting |
|
|
| Underweight |
|
|
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Weight for Age Classification
- There are several classification systems that use weight for age parameter for the classification of protein deficiency.
- These classification; include: Gomez, Jelliffe, IAP, and wellcome-trust classification systems.
- The most commonly used is; Wellcome-Trust/International Classification.
| Welcome Classification: uses both the weight for age and the presence of edema to classify protein energy deficiency disorders. | ||
|---|---|---|
| Weight for age % | Presence of Symmetrical edema | Diagnosis |
| >80% | Positive | Kwashiorkor Nutritional edema |
| 60-80% | Positive | Kwashiorkor |
| Negative | Simple Underweight | |
| <60% | Positive | Kwashiorkor |
| Negative | Marasmus | |
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Weight for Height, and Height for Age Classification
| Water Classification: uses WHO growth charts in reference to the 50th Centile | |
| Weight for height | Degree of Wasting |
| 80-89 | Mild |
| 79-70 | Moderate |
| <70 | Severe |
| Height for age | Degree of Stunting |
| 90-94 | Mild |
| 89-85 | Moderate |
| <85 | Severe |
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Acute Malnutrition Disorders
- Malnutrition definition: acute deficiency of one or more nutritional elements regardless of the total caloric intake, for example: protein deficiency, vitamin deficiency.
- The WHO, and UNICEF define severe acute malnutrition for children between the ages of 6 months to 60 months, as the following;
- Weight for height is below 3 standard deviation score of the median WHO growth standards.
- Visible severe wasting, Bipedal edema, and Mid upper arm circumference below 115mm.
- There are two main categories for malnutrition disorders:
- Kwashiorkor
- Marasmus
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
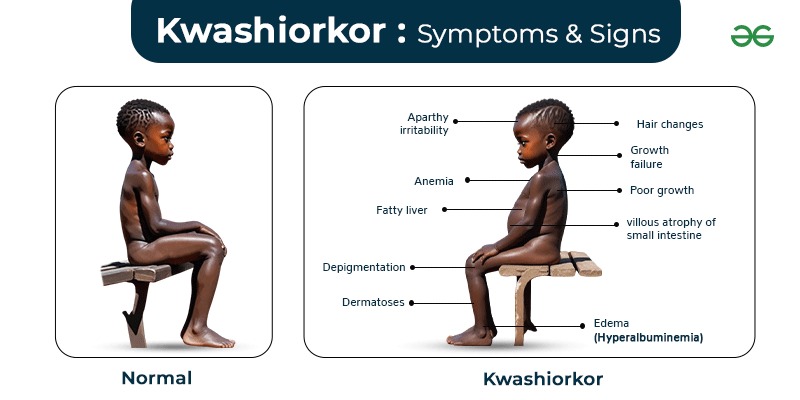
↳ Kwashiorkor (KWO)
- Definition
- A malnutrition disorder characterized by acute protein energy deficiency with normal or high caloric intake.
- Etiology
- Primary Kwashiorkor
- Inadequate diet that does not cover the protein energy requirements of an otherwise healthy patient
- It’s the most common etiology worldwide
- Secondary Kwashiorkor
- Occurs in the settings of a pathology or disease that causes decreased protein intake, decreased absorption or utilization, increased nutritional losses, or increased energy expenditure.
- Primary Kwashiorkor
- Pathophysiology
- Acute protein deficiency leads to a series of reductive adaptation processes in the several body systems.
- These changes are less prominent in marasmus compared to kwashiorkor
- These mechanisms include the following:
-
Pathophysiology Cardiovascular System - Degenerative changes in cardiac muscle
Musculoskeletal System - Degenerative changes in muscle proteins to compensate for the drop in plasma proteins
- Reduction in bone mass and delayed growth
Gastrointestinal System - Atrophy of the intestinal villi, with decreased level of enzymes responsible for digestion and absorption
Hepatobiliary System - Fatty infiltration(steatosis)
- Atrophy of the pancreatic acini causing steatorrhea
Central Nervous System - Slow brain tissue atrophy, and decreased cognitive function
-
- Clinical Features
-
Feature Etiology Signs and Symptoms Edema/Swelling - Decreased plasma proteins →hypoalbuminemia →decreased oncotic pressure →fluid shift from IVC to EVC
- Increased ADH →water retention
- Decreased inactivation of Aldosterone →salt and water retention
- Progressive bilateral, pitting edema
- Starts in the dorsal aspect of both arms and feet, the progress gradually to involve the face (prominent cheeks, moon face)
Growth Faltering/Retardation - Decreased protein intake cause weight loss masked by edema
- Length/Height is less likely to be affected
- Preserved Subcutaneous fat
Muscle Wasting - Degenerative changes of the muscle protein to compensate for the low plasma proteins
- Decreased mid arm and chest circumference
Hair changes - Hair changes are due to amino acid tyrosine deficiency and Copper deficiency necessary for melanin synthesis
- Dry,brittle, easily epilated hair with progressive lightening of color
Skin Changes - Vitamins, Fatty acid, and zinc deficiency
- Dry scaling skin with hyperpigmentation and desquamations
- Skin infection
Gastrointestinal Changes - High carbohydrate diet cause the accumulation of glycogen in the liver
- Fatty infiltration of the liver due to increased fatty acid synthesis
- Infectious and non infectious diarrhea
- Malabsorption
- Hepatomegaly with no cirrhosis
- Abdominal distension
- Diarrhea
Hematological Changes - Iron,protein , folic acid, B12 deficiency
- Prothrombin deficiency
- Anemia ranging from microcytic to macrocytic
- Bleeding tendency
Vitamin Deficiencies - A,B complex, D, and K
- Features discussed in details in Vitamin Deficiencies Lectures
Behavioral Changes - Decreased production of serotonin, nicotinic acid, and adrenergic neurotransmitters
- Apathetic, anorexic, depression, anhedonia
-
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
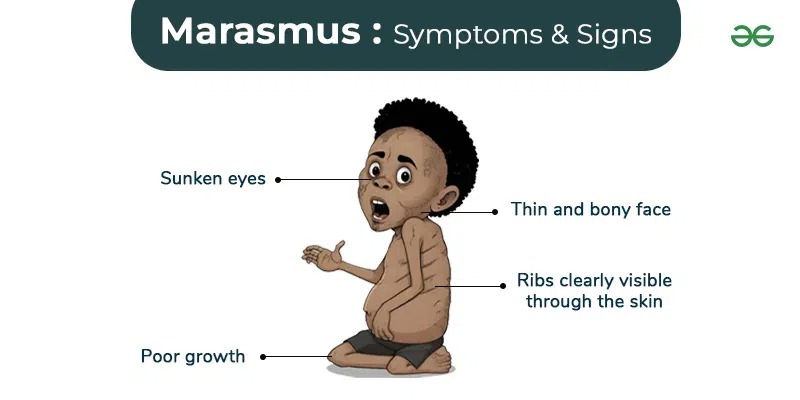
Marasmus (non edematous Protein Calorie Malnutrition)
- Definition
- Severe wasting due to nutritional deficiency of both protein, and total caloric intake.
- Etiology
-
Type Age Cause Primary - 6m-24m
- Decreased amount/frequency of feeds
- Prolonged exclusive breast feedings
Secondary - >24m
- Inability to feed due to illness
- Recurrent gastroenteritis, chronic diarrhea
- Malabsorption syndromes
- Chronic infections
- Prematurity
- Twins
- Congenital anomalies
- Metabolic disorders
- Child abuse
- Edncorinopathies
- Malignancies
-
- Clinical Features
- Muscle wasting
- Degenerative changes of the muscle protein to compensate for the low plasma proteins.
- Loss of subcutaneous fat
- Prominent costochondral junctions (false rosaries).
- Hypothermia <35.5C
- Scaphoid, distended Abdomen
- Absence of edema
- Zinc Deficiency
- acrodermatitis enteropathica: rash, alopecia, diarrhea, recurrent infections
- Muscle wasting
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Complications of Malnutrition Disorders
- Dehydration
- Electrolyte Disturbances
- Recurrent Infections and Septic Shock
- Hypothermia
- Heart Failure
- Failure to Thrive
- Death
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Diagnosis of Malnutrition Disorders
- Rule out primary causes of marasmus.
- If a secondary cause is suspected, laboratory tests and radiological imaging are used to identify the cause.
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Management of Acute Severe Malnutrition Disorders
- Treatment generally progresses through three phases: Stabilization phase, Rehabilitation preparation, and Rehabilitation phase.
- The duration of management varies according to severity, and continues until the child’s weight is back to normal levels (6-8 weeks).
| Phases of Management | ||
|---|---|---|
| Initial Phase (Stabilization Phase) | ||
| Duration | Objectives | Management |
|
|
|
| Transition Phase (Rehabilitation Preparation) | ||
| Duration | Objectives | Management |
|
|
|
| Phase 3 Title (Rehabilitation Phase) | ||
| Duration | Objectives | Management |
|
|
|
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Refeeding Syndrome after Acute Malnutrition Treatment
- Definition
- A life-threatening condition that occurs during the reintroduction of nutrition to individuals after prolonged starvation or severe malnutrition.
- It is a state of metabolic and electrolyte disturbances, particularly involving shifts in phosphorus, potassium, magnesium, glucose, and fluids.
- Pathophysiology:
- During the starvation or severe malnutrition Phase
- The body consumes its own stores of minerals, and nutrients, with decreased insulin secretion.
- Intracellular minerals (phosphate, potassium, and magnesium) stores are depleted but remain normal in the serum due to the lack of insulin-driven intracellular shift.
- During the refeeding Phase
- The rapid, and sudden intake of carbohydrates cause an insulin surge to facilitate glucose metabolism.
- Insulin release leads to the rapid uptake of glucose, potassium, magnesium, and phosphate into the cells, which lowers their serum levels.
- These sudden intracellular shifts cause fluid retention, electrolyte imbalances, and an overall systematic dysfunction.
- During the starvation or severe malnutrition Phase
- Clinical Picture
- The clinical signs and symptoms of refeeding syndrome are variable, but typical begin within 3-5 days of initiating refeeding.
Clinical Features Electrolyte Disturbances - Hypophosphatemia: muscle weakness and pain, rhabdomyolysis, respiratory failure.
- Hypokalemia: Cardiac arrhythmias, muscle weakness and cramps.
- Hypomagnesemia: tetany, arrhythmias, seizures.
Cardiovascular manifestations - Arrhythmias (low potassium and magnesium).
- Congestive heart failure (fluid overload, peripheral edema).
Respiratory manifestations - Respiratory failure (low phosphate levels can weaken the diaphragm and respiratory muscles).
Gastrointestinal manifestations - Nausea, vomiting, diarrhea, and abdominal pain.
Hematological manifestations - Hemolytic anemia ( low phosphate level).
Neurological manifestations - Confusion, irritability, seizures (low magnesium and phosphate).
- The clinical signs and symptoms of refeeding syndrome are variable, but typical begin within 3-5 days of initiating refeeding.
- Treatment
- Correction of Electrolytes with continuous monitoring of levels
- Fluid and Glucose Management
- Vitamin Supplementation
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.
فيديوهات الشرح
بطاقات تفاعلية
أسئلة ممارسة
اشترك الآن