Summary
Celiac disease (also called gluten-sensitive enteropathy or celiac sprue) is an autoimmune disorder of the small intestine triggered by gluten in genetically predisposed individuals (HLA-DQ2 or HLA-DQ8).
- It mainly damages the distal duodenum and proximal jejunum, leading to malabsorption and steatorrhea.
- Patients present with chronic diarrhea, bloating, weight loss, iron deficiency anemia, or failure to thrive in children.
- It is strongly associated with dermatitis herpetiformis, low bone density, and a small increased risk of enteropathy-associated T-cell lymphoma (EATL).
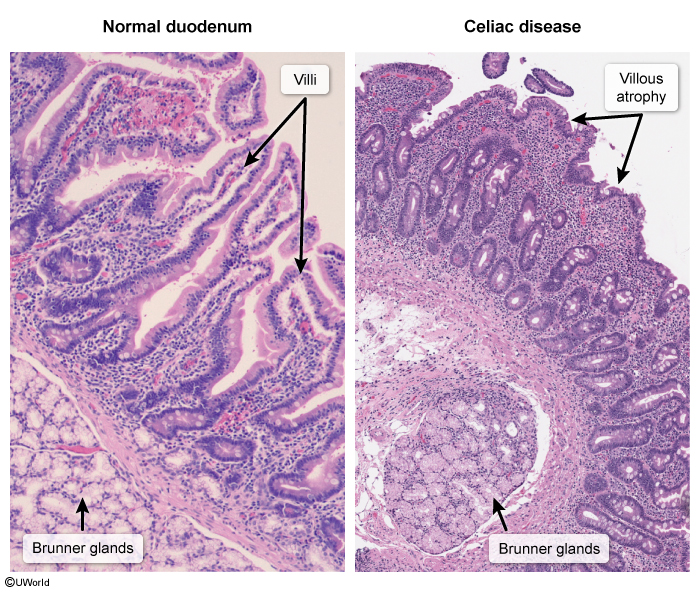
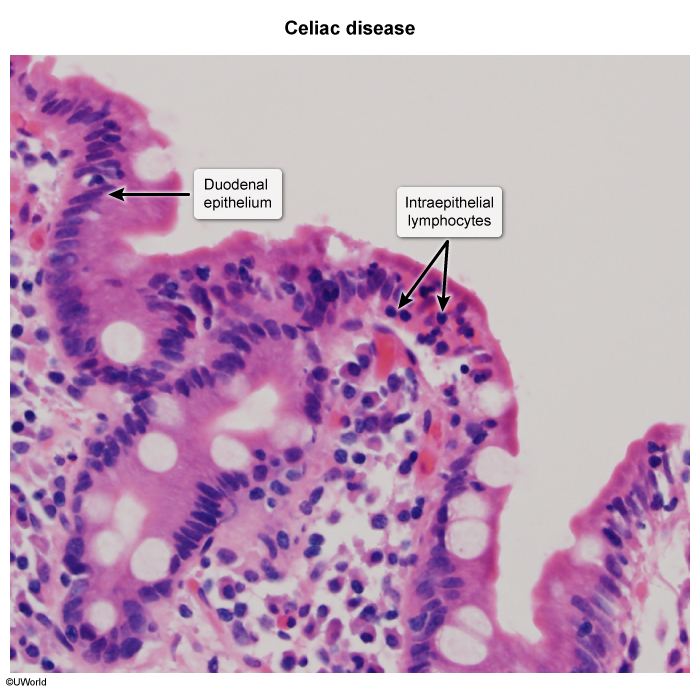
- Histology shows the classic triad: villous atrophy, crypt hyperplasia, and intraepithelial lymphocytosis.
- Treatment is a strict lifelong gluten-free diet plus correction of nutrient deficiencies.
Epidemiology
- More common in North America, Europe, the Middle East, and Australia.
- Prevalence ~1% of the general population; many cases remain undiagnosed.
- Two peaks of presentation:
- Infants (6 months – 2 years): shortly after gluten is introduced into the diet — classic GI symptoms.
- Adults (30s–40s): often with subtle or extraintestinal symptoms (e.g., isolated iron deficiency anemia).
- Female predominance (~2:1).
- Strong genetic link: nearly all patients carry HLA-DQ2 (~90%) or HLA-DQ8 (~5–10%).
- Higher prevalence in patients with Down syndrome, Turner syndrome, type 1 diabetes, and first-degree relatives of celiac patients.
Etiology and Pathogenesis
Celiac disease is an autoimmune reaction triggered by gluten, a storage protein found in:
- Wheat
- Rye
- Barley
- Oats (cross-contamination; pure oats tolerated by most)
| Gluten Sources — "BROW" | |
| Barley • Rye • Oats • Wheat Genetics → "Celiac = DQ 2 or 8" (HLA-DQ2 / HLA-DQ8) |
جملة تذكرية |
Step-by-step pathogenesis
- Dietary gluten is partially digested to gliadin in the gut lumen.
- Gliadin crosses the intestinal epithelium and is deamidated by the enzyme tissue transglutaminase (tTG) in the lamina propria.
- Deamidated gliadin is presented by HLA-DQ2 or HLA-DQ8 on antigen-presenting cells to CD4+ T helper cells.
- Activated T cells release pro-inflammatory cytokines (IFN-γ) that recruit intraepithelial lymphocytes and damage the mucosa → villous atrophy.
- B cells produce autoantibodies: anti-tTG IgA, anti-endomysial IgA (EMA), and anti-deamidated gliadin peptide (DGP).
The end result is loss of absorptive surface area → malabsorption of nutrients, fats, and vitamins.
Associated condition: Selective IgA deficiency is the most commonly linked immunodeficiency — important because it can cause false-negative IgA-based serology.
Clinical Features
Celiac disease has a wide range of presentations — from classic GI symptoms in children to silent or extraintestinal disease in adults. See the multisystem clinical manifestations table for a complete organ-system breakdown.
Gastrointestinal symptoms
- Chronic diarrhea ± steatorrhea (bulky, foul-smelling, greasy, floating stools).
- Abdominal pain, bloating, flatulence.
- Weight loss in adults; failure to thrive in children.
- Nausea, vomiting, or constipation (less common).
Extraintestinal manifestations
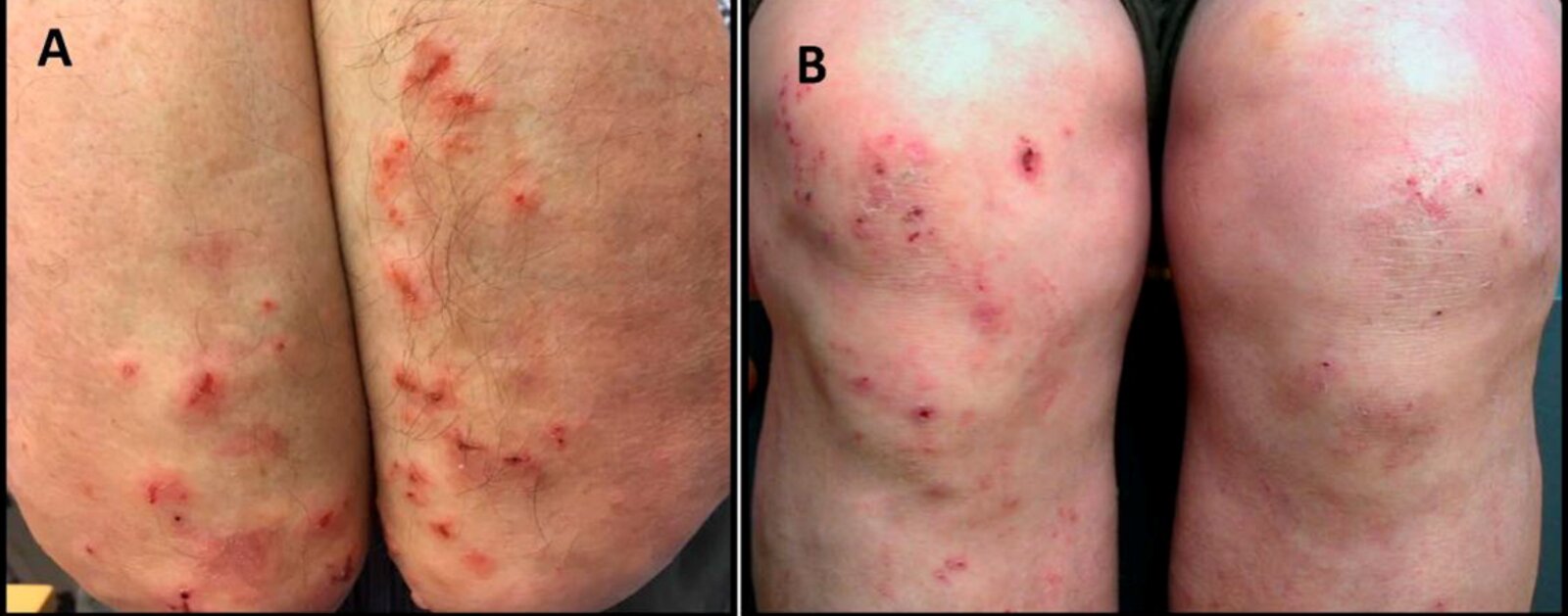
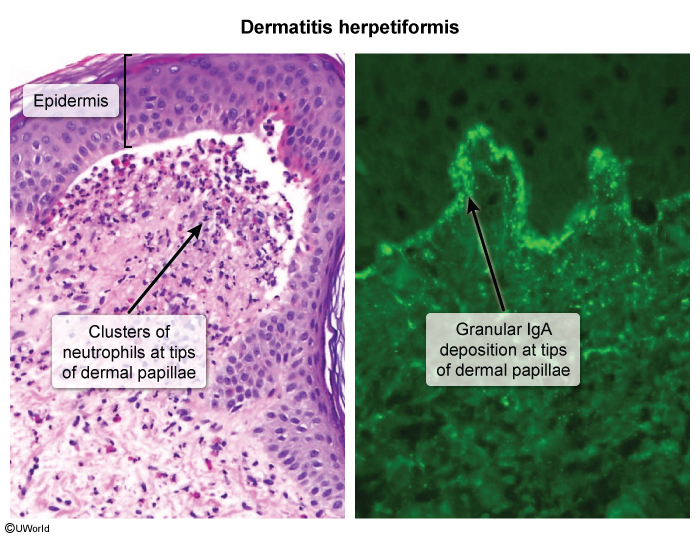
- Dermatitis herpetiformis — intensely pruritic, grouped papulovesicles on extensor surfaces (elbows, knees, buttocks). Seen in 10–25% of patients. Caused by IgA deposits in the dermal papillae.
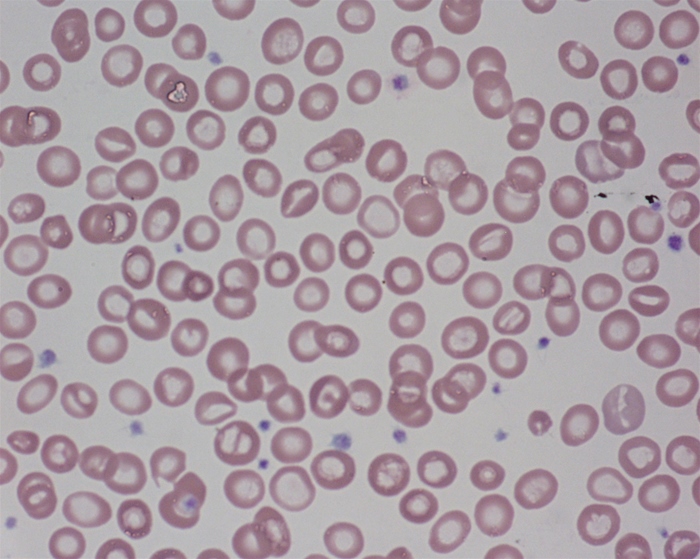
- Iron deficiency anemia — often the only sign in adults; may not respond to oral iron due to duodenal malabsorption.
- Osteopenia / osteomalacia — from vitamin D and calcium malabsorption.
- Atrophic glossitis, aphthous stomatitis.
- Easy bruising — vitamin K deficiency → prolonged PT/INR.
- Peripheral neuropathy, depression, anxiety.
- Short stature, delayed puberty in children.
Features of Malabsorption
Because the proximal small bowel is the main site of nutrient absorption, celiac disease leads to a wide variety of deficiencies. Each missing nutrient produces a distinct clinical sign — see also the full malabsorption reference table and the nutrient deficiency overview.
| Malabsorption — Nutrient Deficiencies in Celiac Disease | |
|---|---|
| Nutrient lost | Clinical sign |
| Fat & protein | Steatorrhea, muscle wasting, edema (hypoalbuminemia) |
| Iron | Microcytic hypochromic anemia, pallor, fatigue |
| Calcium + Vitamin D | Osteomalacia / rickets, bone pain, pathologic fractures |
| Vitamin K | Easy bruising, prolonged PT/INR |
| Vitamin A | Hyperkeratosis, night blindness |
| Folate | Macrocytic (megaloblastic) anemia |
| Vitamin B12 | Neuropathy — less common (absorbed in terminal ileum) |
| Iron vs. Folate in Celiac | |
| Celiac disease primarily affects the proximal small bowel (duodenum/jejunum) → iron and folate are most commonly deficient. B12 is absorbed in the terminal ileum and is usually spared unless disease is extensive. |
تذكر |
Diagnosis
Diagnosis follows a stepwise approach. The patient must be on a gluten-containing diet during testing — otherwise results may be falsely negative. See the celiac disease symptoms, signs & diagnosis table.
Step 1 — Serology (screening)
- Anti-tissue transglutaminase IgA (anti-tTG IgA) → first-line, most sensitive & specific.
- Anti-endomysial antibody (EMA) IgA → highly specific confirmatory test.
- Total serum IgA → always check to rule out IgA deficiency (causes false-negative tTG).
- If IgA deficient → switch to IgG-based tests: deamidated gliadin peptide IgG (DGP-IgG) or tTG-IgG.
Step 2 — Duodenal biopsy (gold standard)
An EGD with ≥4 biopsies from the distal duodenum (+ 1–2 from the bulb) confirms the diagnosis. Histology shows the classic triad:
- Villous atrophy — flattened villi reduce absorptive surface.
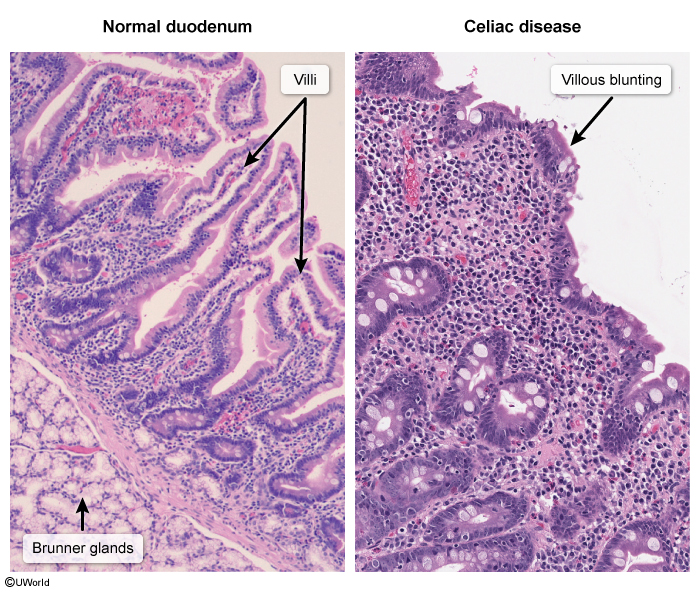
- Crypt hyperplasia — elongated crypts (compensatory proliferation).
- Intraepithelial lymphocytosis — >25 lymphocytes per 100 enterocytes (earliest finding).
The presence of Brunner glands in the biopsy confirms the duodenal location of the sample.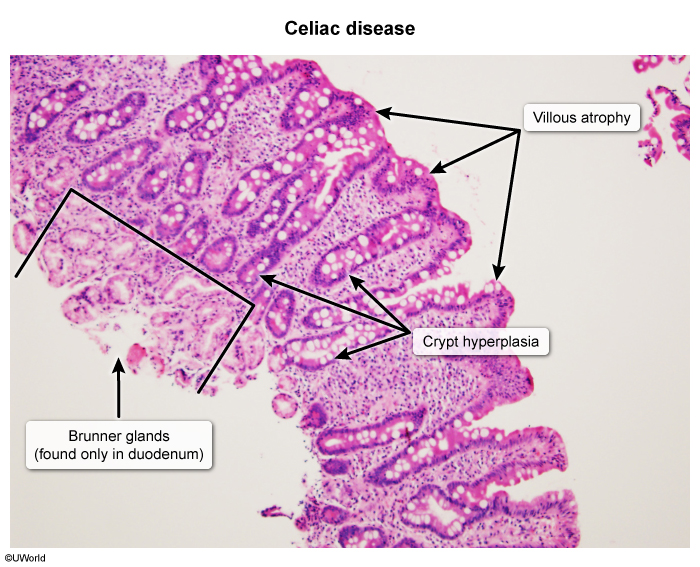
Step 3 — Response to gluten-free diet
Resolution of symptoms, normalization of antibodies, and improved villous architecture on follow-up biopsy confirm the diagnosis.
| Classic Exam Scenario — فكرة سؤال | |
| An adult presents with unexplained iron deficiency anemia not responding to oral iron → always consider celiac disease! Order: anti-tTG IgA + total serum IgA. |
تذكر |
Differential Diagnosis
Many GI conditions mimic celiac disease. The combination of chronic diarrhea + nutrient deficiencies + positive serology + villous atrophy on biopsy distinguishes celiac from the alternatives below. For patients with diarrhea-predominant symptoms, also see the malabsorption syndromes comparison.
| Differential Diagnosis of Celiac Disease | |
|---|---|
| Condition | Key distinguishing feature |
| Lactose intolerance | Bloating/diarrhea after dairy; normal biopsy; H₂ breath test (+) |
| Crohn disease | Bloody stools, fistulae, transmural inflammation; skip lesions; ileal involvement |
| Irritable bowel syndrome | Alternating bowel habits; NO weight loss, anemia, or villous atrophy; Rome IV criteria |
| Tropical sprue | Travel to tropics; responds to antibiotics + folate; involves entire small bowel |
| Whipple disease | Arthralgia, CNS/cardiac signs; PAS-positive macrophages on biopsy |
| Chronic pancreatitis | Steatorrhea + diabetes; epigastric calcifications on imaging |
| Small intestinal bacterial overgrowth | Bloating, diarrhea; predisposing conditions (scleroderma, surgical blind loops); H₂ breath test |
Causes of steatorrhea — reference table
Treatment
See the management of celiac disease — full table for a complete reference.
1. Strict, lifelong gluten-free diet (cornerstone)
- Avoid wheat, rye, barley. Most patients tolerate pure oats.
- Safe alternatives: rice, corn, potatoes, quinoa, buckwheat.
- Patients should read all food labels — gluten hides in sauces, processed meats, and some medications.
- Symptoms usually improve within weeks; mucosal healing takes months to years.
2. Correct nutrient deficiencies
- Iron, folate for anemia (most common deficiencies).
- Calcium + vitamin D for bone health; order a DXA scan at diagnosis to screen for osteomalacia/osteoporosis.
- Vitamin K, A if clinically deficient.
3. Specific therapies
- Dermatitis herpetiformis → gluten-free diet ± dapsone for rapid skin relief.

- Pneumococcal vaccination — celiac patients have functional hyposplenism.
- Follow-up serology (anti-tTG IgA) at 6 and 12 months to confirm dietary adherence.
4. Refractory celiac disease
Persistent symptoms despite a strict gluten-free diet → work through the differential systematically:
| Refractory Symptoms — فكرة سؤال | |
| If a patient on a gluten-free diet still has symptoms, the most common cause is hidden gluten exposure — not true refractory sprue. Rule out: hidden gluten → lactose intolerance → microscopic colitis → SIBO → then consider refractory celiac or EATL. |
تذكر |
Complications and Associated Conditions
Complications
- Iron deficiency anemia — most common complication overall.
- Osteoporosis / osteomalacia — from calcium and vitamin D malabsorption → increased fracture risk.
- Infertility, recurrent miscarriage — reversible with gluten-free diet.
- Growth failure and delayed puberty in children.
- Enteropathy-associated T-cell lymphoma (EATL) — rare but feared; risk increases with poor dietary compliance.
- Small bowel adenocarcinoma — slightly increased risk.
- Ulcerative jejunitis, refractory sprue.
Associated autoimmune disorders
- Type 1 diabetes mellitus — shared HLA associations; screen celiac patients and vice versa.
- Autoimmune thyroid disease (Hashimoto, Graves).
- Selective IgA deficiency — remember: can cause false-negative serology.
- Down syndrome, Turner syndrome — increased prevalence; screen routinely.
- Primary biliary cholangitis, autoimmune hepatitis.
Dermatitis herpetiformis — the skin manifestation
Skin conditions and associated systemic diseases — DH is the pathognomonic skin finding of celiac disease, caused by granular IgA deposits at dermal papillae. Biopsy of perilesional skin with direct immunofluorescence showing granular IgA is diagnostic.
Mnemonics
| The Whole Disease in One Word — "CELIAC" | |
| C — Chronic diarrhea & malabsorption E — Extraintestinal: anemia, DH, osteoporosis L — HLA-DQ2 / DQ8 genetics ("L" = Linkage) I — Intraepithelial lymphocytes + IgA tTG A — Atrophy of villi + crypt hyperplasia C — Cure = gluten-free diet for life |
جملة تذكرية |
Key Points for Exams – نقاط مهمة للامتحانات
- Trigger: Gluten (wheat, rye, barley) → BROW.
- Genetics: HLA-DQ2 (~90%) or HLA-DQ8.
- Site affected: Distal duodenum / proximal jejunum.
- Histology triad: Villous atrophy + crypt hyperplasia + intraepithelial lymphocytosis.
- Earliest histologic finding: Intraepithelial lymphocytosis (>25 lymphocytes per 100 enterocytes).
- Best initial test: Anti-tTG IgA (+ total serum IgA to rule out IgA deficiency).
- Gold standard: Duodenal biopsy while patient is on a gluten-containing diet.
- Classic skin sign: Dermatitis herpetiformis → treat with gluten-free diet ± dapsone.
- Adult presentation clue: Iron deficiency anemia not responding to oral iron.
- Treatment: Lifelong gluten-free diet + vitamin/mineral replacement + pneumococcal vaccine.
- Malignancy risk: Enteropathy-associated T-cell lymphoma (EATL).
- Associations: Type 1 DM, autoimmune thyroid disease, IgA deficiency, Down syndrome, Turner syndrome.
Celiac disease — comprehensive reference table · Risk factors, symptoms, diagnosis & treatment
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.