Summary
Preeclampsia and eclampsia are hypertensive disorders of pregnancy with significant maternal and fetal risks. Preeclampsia is defined by new-onset hypertension with proteinuria or end-organ dysfunction after 20 weeks, while eclampsia is characterized by seizures complicating preeclampsia. Management centers on maternal stabilization, seizure and BP control, and timely delivery, with postpartum monitoring and recurrence prevention strategies. Early recognition, vigilant monitoring, and appropriate interventions remain critical to reducing maternal and perinatal morbidity and mortality.
Introduction
Preeclampsia and eclampsia are major hypertensive disorders of pregnancy, representing leading causes of maternal and perinatal morbidity and mortality worldwide. Preeclampsia is defined as new-onset hypertension (≥140/90 mmHg) after 20 weeks’ gestation with proteinuria or evidence of end-organ dysfunction, whereas eclampsia is characterized by the occurrence of seizures in a preeclamptic patient in the absence of other neurological or metabolic causes. Preeclampsia complicates 5–7% of pregnancies, while eclampsia occurs in <0.1% of deliveries but carries a high maternal (≈1.8%) and fetal (≈30%) mortality rate.
Pathophysiology
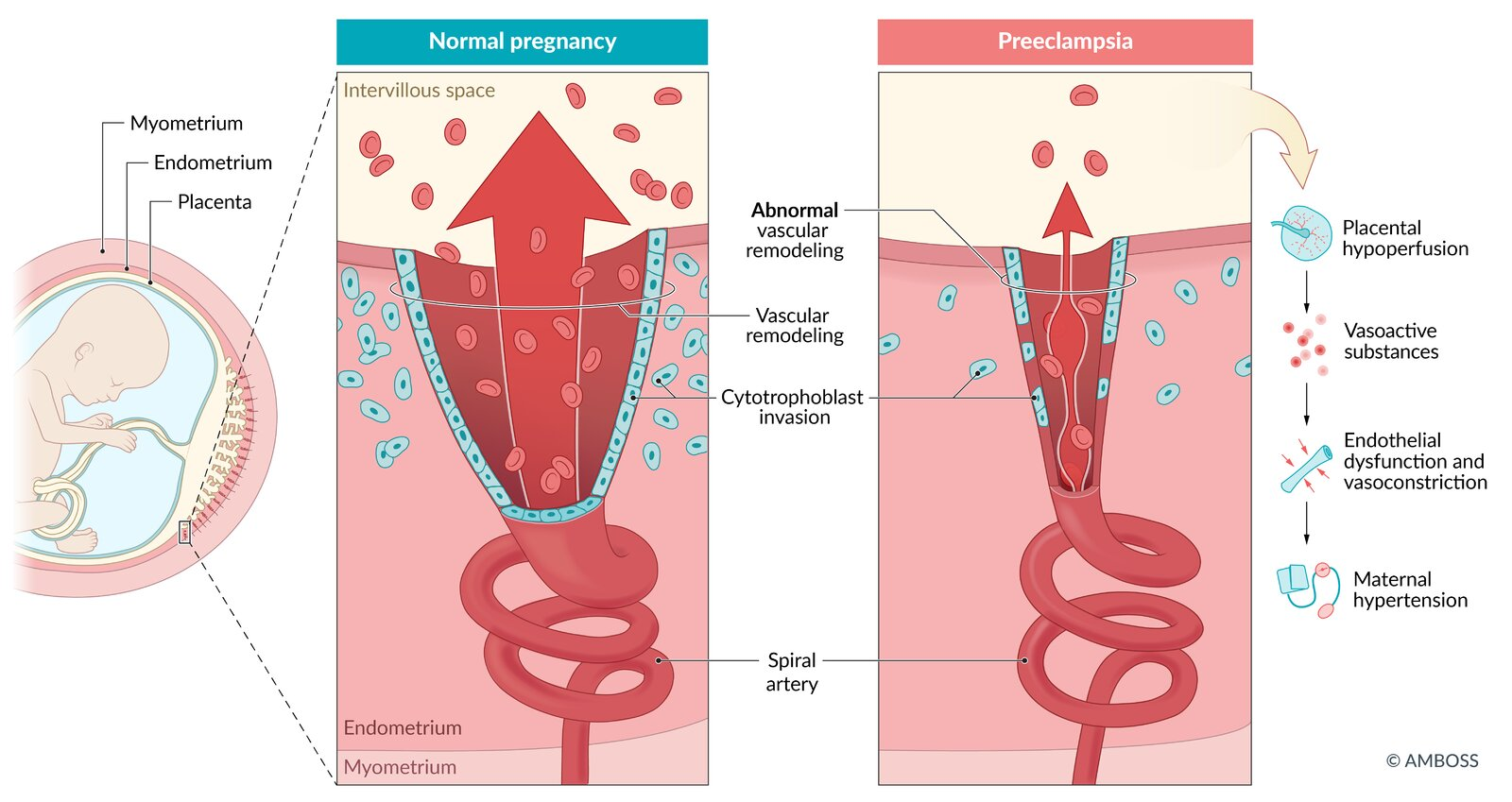
Preeclampsia is a placental disorder caused by abnormal trophoblastic invasion of the spiral arteries, leading to incomplete remodeling and a high-resistance, low-flow uteroplacental circulation. This results in hypoxia, oxidative stress, systemic inflammation, and endothelial dysfunction, producing hypertension, proteinuria, and multi-organ involvement.
-
Preeclampsia: multiorgan dysfunction, predominantly renal.
-
Eclampsia: cerebral involvement with seizures.
-
HELLP syndrome: microangiopathic hemolysis, hepatic involvement, and thrombocytopenia.
Risk Factors
Risk factors are divided into moderate and high-risk categories (Table 1). Prophylactic low-dose aspirin (75–150 mg daily) from 12 weeks’ gestation is recommended for women with ≥1 high-risk or ≥2 moderate-risk factors.
Risk Factors for Preeclampsia:
|
Moderate Risk Factors |
High Risk Factors |
|
Nulliparity |
Previous preeclampsia/eclampsia |
|
Maternal age ≥40 |
Chronic hypertension |
|
BMI ≥35 |
Diabetes mellitus (T1DM/T2DM) |
|
Family history of preeclampsia |
Chronic kidney disease |
|
Pregnancy interval >10 years |
Autoimmune disease (SLE, APS) |
|
Multiple pregnancy |
Multifetal gestation |
Clinical Features
Preeclampsia
-
Without severe features: Hypertension, proteinuria, headache, visual changes, edema.
-
With severe features: Severe hypertension (≥160/110 mmHg), thrombocytopenia (<100,000/mm³), impaired renal or liver function, pulmonary edema, cerebral or visual disturbances.
-
HELLP syndrome: Hemolysis, elevated liver enzymes, low platelets; may occur without hypertension or proteinuria.
Eclampsia
-
Generalized tonic-clonic seizures (60–75 seconds, followed by postictal state).
-
Warning signs: persistent headache, hyperreflexia, visual disturbances, right upper quadrant/epigastric pain.
-
Seizure timing: postpartum (44%), antepartum (38%), intrapartum (18%).
Complications
Complications of Preeclampsia and Eclampsia:
|
Maternal Complications |
Fetal Complications |
|
HELLP syndrome |
Intrauterine growth restriction (IUGR) |
|
Acute kidney injury |
Preterm birth |
|
Disseminated intravascular coagulation (DIC) |
Intrauterine fetal death |
|
Pulmonary edema / ARDS |
Placental abruption |
|
Cerebrovascular hemorrhage |
Neonatal respiratory distress |
|
Permanent CNS damage |
Stillbirth |
|
Maternal death |
Differential Diagnosis
Conditions that may mimic preeclampsia/eclampsia include:
-
For hypertension: chronic hypertension, gestational hypertension, renal disease.
-
For seizures: epilepsy, hypoglycemia, intracranial hemorrhage, meningitis, brain tumor, metabolic disorders.
-
For HELLP syndrome: acute fatty liver of pregnancy, intrahepatic cholestasis, thrombotic thrombocytopenic purpura (TTP), hemolytic uremic syndrome (HUS), viral hepatitis.
Investigations
-
Blood tests: FBC (↓platelets, anemia), renal function (↑urea, ↑creatinine, ↑urate), LFTs (↑AST/ALT), coagulation profile.
-
Urine tests: proteinuria (24h collection ≥300 mg, protein:creatinine ratio ≥0.3).
-
Imaging: Obstetric ultrasound (growth, placental abruption), CT/MRI if neurological cause suspected.
-
Fetal monitoring: Cardiotocography (CTG) for distress/bradycardia.
Management
General Principles
-
Stabilize the mother: ABCDE approach, left lateral position, oxygen.
-
Seizure control (eclampsia): Magnesium sulfate is first-line (loading 4 g IV, maintenance 1 g/h for 24 h; additional 2 g bolus if recurrent). Monitor for hypermagnesemia (loss of reflexes, respiratory depression).
-
Blood pressure control: IV labetalol or hydralazine; target MAP <120 mmHg. Avoid rapid BP reduction.
-
Delivery: The only definitive treatment. Once the mother is stabilized, proceed to delivery irrespective of gestational age. Caesarean section is often preferred unless vaginal delivery is imminent.
-
Monitoring: Strict fluid balance, urine output, serial labs (platelets, creatinine, transaminases).
Postpartum Care
-
Continue magnesium sulfate for 24 hours after last seizure/delivery.
-
Monitor BP daily for 2–3 days, then at 3–5 days postpartum.
-
Reassess for antihypertensive needs.
-
6-week follow-up: check BP, proteinuria, renal and liver function.
-
Counsel regarding recurrence risk and aspirin prophylaxis in future pregnancies.
Prevention
-
Address modifiable risk factors preconceptionally (weight, comorbidities, smoking cessation).
-
Screen at every antenatal visit for hypertension and proteinuria.
-
Low-dose aspirin prophylaxis (75–150 mg from 12–20 weeks until delivery) in high-risk women.
-
Calcium supplementation in populations with low dietary intake.
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.