شرح المدرسين

Introduction
Also known as operative vaginal birth, involves the use of instruments such as forceps or a vacuum device to help extract the fetus through the vagina during childbirth. This method may be employed with or without the mother's efforts in pushing. The decision to proceed with an assisted vaginal birth takes into consideration the potential impacts on the mother, fetus, and newborn, comparing these risks with those associated with cesarean birth or opting for expectant management.
Indications
- Maternal exhaustion leading to an inability to push effectively.
- Maternal medical conditions that necessitate minimizing the exertion of pushing, such as cardiac diseases.
- Prolonged second stage of labor, where the labor does not progress as expected.
- Fetal concerns that indicate immediate or impending compromise, suggesting that expedited delivery is necessary for the well-being of the fetus.
Contraindications
- Extreme fetal prematurity: Assisted vaginal birth is not recommended due to the heightened vulnerability of premature infants to injury during the birth process.
- Fetal demineralizing diseases: Conditions such as osteogenesis imperfecta, which weaken the bones, make the use of forceps or vacuum birth unsafe due to the increased risk of skull deformation, fracture, and potential brain injuries.
- Fetal bleeding disorders: Conditions like fetal hemophilia or neonatal alloimmune thrombocytopenia pose significant risks for bleeding complications, making assisted vaginal birth hazardous.
- Unengaged fetal head: If the fetal head has not descended into the pelvis (engagement), attempting an assisted vaginal birth could be unsafe.
- Uncertain fetal position: Without clear knowledge of the fetal position, using instruments could pose unnecessary risks.
- Brow or face presentation: These fetal presentations are not suitable for assisted vaginal birth due to the difficulty and risk of injury in guiding the fetus through the birth canal.
- Suspected fetal-pelvic disproportion: If the fetus is suspected to be too large to pass through the maternal pelvis, assisted vaginal birth is contraindicated.
A relative contraindications specific to vacuum extraction, including:
- Gestational age below 34 weeks: The vulnerability of the neonate's scalp and skull at this early gestational age makes vacuum extraction riskier.
- History of scalp sampling: Although rare in modern practice, previous scalp sampling increases the risk of complications with vacuum extraction.
Classification
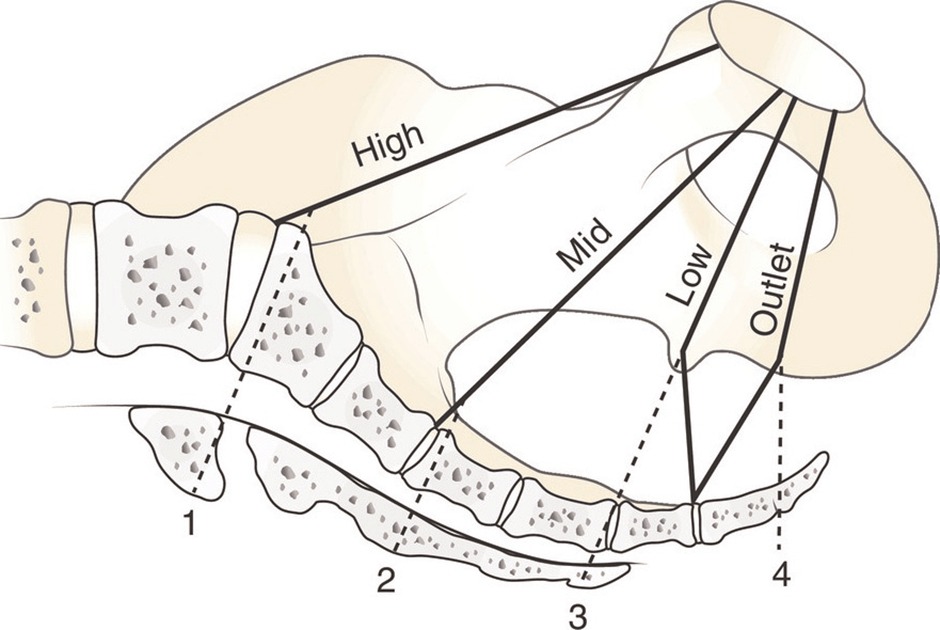
Classification of forceps
The forceps is a metal device that enables gentle rotation and/or traction of the fetal head during vaginal delivery, classification based on the fetal station (the position of the fetal head in relation to the ischial spines of the mother's pelvis) and the degree of head rotation required for delivery.

- Outlet Forceps:
- The fetal skull's leading point has reached the pelvic floor, visible at the introitus without labia separation.
- The sagittal suture is in the anteroposterior diameter or in a right or left occiput anterior or posterior position.
- Rotation does not exceed 45 degrees.
- Low Forceps:
- The leading point of the fetal skull is at least 2 cm beyond the ischial spines but not on the pelvic floor, with the station at least +2/5 cm.
- There are two subcategories based on head rotation:
- Without rotation: Head rotation is 45 degrees or less.
- With rotation: Head rotation is greater than 45 degrees.
- Midforceps:
- The fetal head is engaged (at least 0 station), but the leading point of the skull is not more than 2 cm beyond the ischial spines, with the station between 0 to +1/5 cm.
- The fetal head is engaged (at least 0 station), but the leading point of the skull is not more than 2 cm beyond the ischial spines, with the station between 0 to +1/5 cm.
Classification of Vacuum
The vacuum extractor is a metal or plastic cup, attached to the fetal head with a suction device, that enables traction of the fetal head during vaginal delivery
- Vacuum-assisted births do not have a specific classification system related to station and rotation.
- The station at which the vacuum was applied should be documented.
- Rotational maneuvers with a vacuum are generally avoided to reduce the risk of severe scalp injuries and subgaleal hemorrhage.

The prerequisites
- Cervical Dilation: The cervix must be fully dilated to allow for the safe passage of the fetus.
- Membrane Status: The membranes must be ruptured, which often occurs naturally during labor or may be performed artificially by the healthcare provider.
- Fetal Head Engagement: The fetal head must be engaged, indicating it has descended into the maternal pelvis to at least 0/5 cm station. This is crucial to avoid applying instruments when the head is not properly positioned.
- Accurate Assessment of Fetal Position: It's vital to know the fetal presentation, position, station, and any asynclitism. The fetus should be in a cephalic presentation, except in specific scenarios like using Piper forceps for a breech presentation.
- Fetal Size Considerations: The fetus should not be too large or too small for the type of delivery planned, taking into account the maternal pelvic structure and the fetal size.
- Pelvic Assessment: Clinical pelvimetry should indicate an adequate pelvis size relative to the estimated fetal size, considering factors like the sacrum's shape, subpubic angle, and the distance between the ischial spines.
- Informed Consent: The patient must consent to the procedure, with an understanding of the reasons, risks, benefits, and alternatives.
- Cesarean Birth Readiness: There must be immediate availability to perform a cesarean birth if complications arise during the assisted vaginal delivery.
- Anesthesia: Adequate anesthesia should be provided to ensure the patient's comfort and cooperation during the procedure.
- Empty Bladder: The maternal bladder should be empty to maximize space for fetal descent and reduce the risk of bladder injury.
- Willingness to Abandon the Procedure: The healthcare provider must be prepared to stop the procedure if it becomes clear that it cannot be safely or effectively completed.
Choices of instruments
- Vacuum versus Forceps:
- Vacuum extraction is often selected when an easier extraction is anticipated, such as in cases where the fetus is in an occipito-anterior position at low stations without signs of relative cephalopelvic disproportion.
Vacuum extraction is generally less traumatic for the mother, easier to apply, requires less maternal anesthesia, and allows for passive fetal head rotation during extraction. - Forceps are chosen when a difficult extraction is anticipated, despite the slightly higher risk of maternal injury, because they have a higher success rate, can actively rotate the fetal head, and are unlikely to detach during extraction.
Forceps can be used on preterm fetuses and do not exacerbate bleeding from scalp lacerations.
- Vacuum extraction is often selected when an easier extraction is anticipated, such as in cases where the fetus is in an occipito-anterior position at low stations without signs of relative cephalopelvic disproportion.
- Choice of Vacuum Cup:
- Soft vacuum cups are suited for most births, particularly outlet deliveries in the occiput anterior position, as they are associated with less scalp trauma.

- Rigid cups may be preferred for more challenging deliveries, such as occiput posterior, occiput transverse, and difficult occiput anterior deliveries, due to their lower likelihood of detachment.
- Soft vacuum cups are suited for most births, particularly outlet deliveries in the occiput anterior position, as they are associated with less scalp trauma.
- Choice of Forceps:
The selection of forceps is based on the size and shape of the fetal head and maternal pelvis, the fetal head position and station, and whether rotation is planned.- Simpson type forceps fit well for a molded head due to their less concave cephalic curve.

- Elliott type forceps or Tucker-McLane type forceps are better for a round, unmolded head.

- Kielland forceps are useful for rotations because of their minimal pelvic curve and sliding lock, which is advantageous in the presence of asynclitism.

- Piper forceps are specifically designed for assisting the birth of the aftercoming head in vaginal breech deliveries.

- Simpson type forceps fit well for a molded head due to their less concave cephalic curve.
The procedure
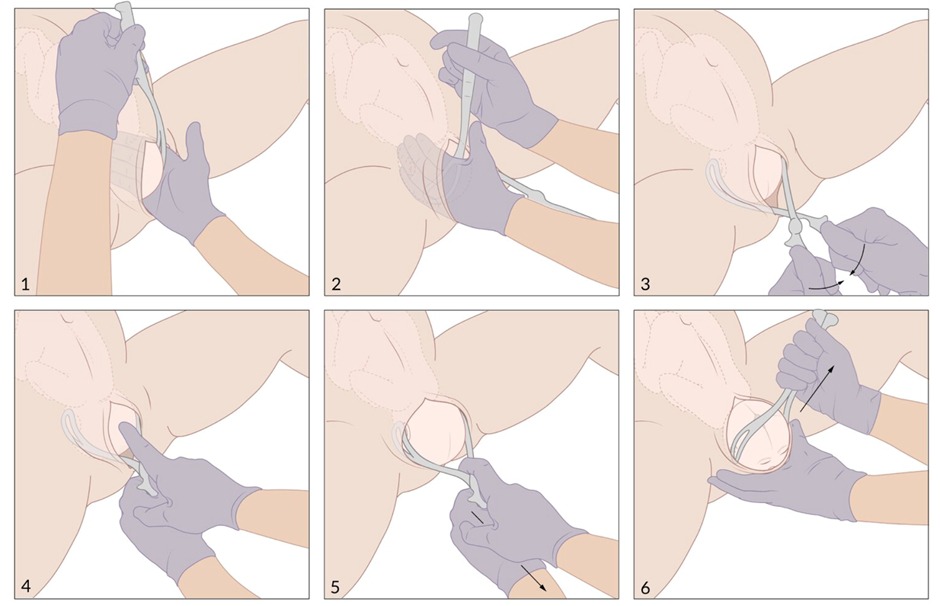
Forceps Delivery
- Application: Proper application of forceps involves aligning the blades with the fetal head's occipitomental diameter, ensuring the sagittal suture is bisected evenly by the blades, and avoiding maternal tissue entrapment.
- Midforceps Births: Generally avoided due to higher risks of maternal and fetal complications. They may be considered in emergencies if performed by highly experienced clinicians.
- Rotation and Traction: Rotation is executed between contractions if needed. Traction should be steady, in line with the birth canal, and synchronized with maternal efforts.
- Removal: Forceps are removed once the fetal head is about to be delivered to reduce laceration risks.
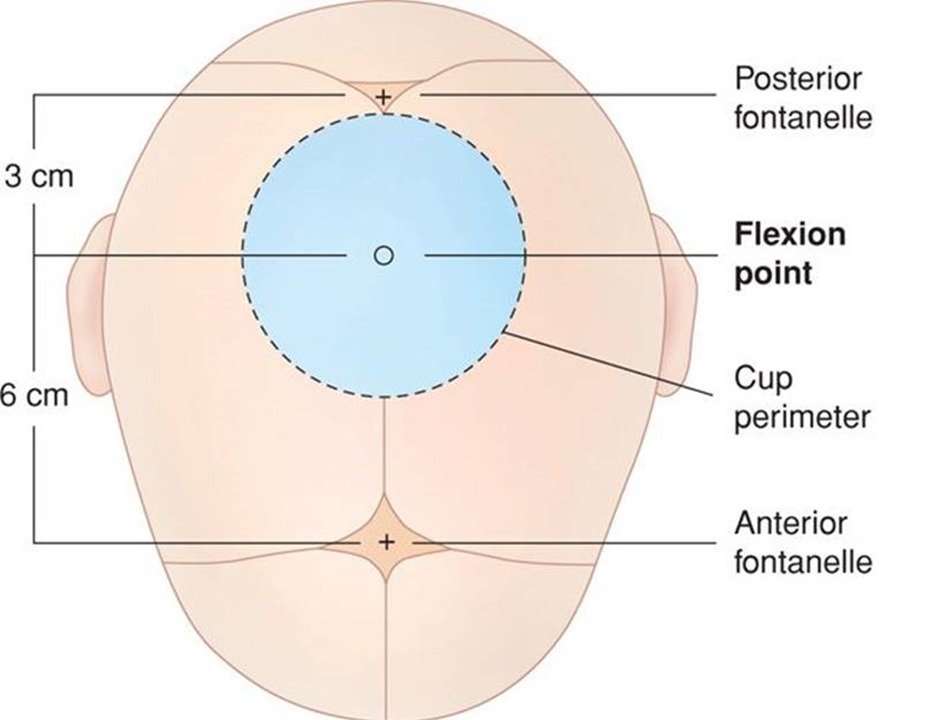
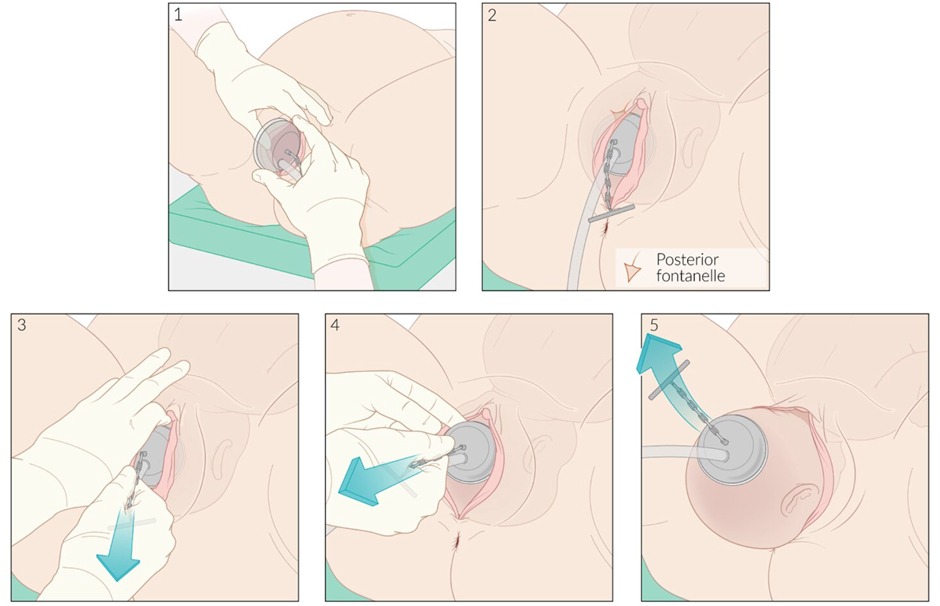
Vacuum Extraction
- Detailed separately, vacuum extraction involves attaching a cup to the fetal head at the flexion point and applying suction to assist with delivery.
When to Abandon the Procedure
The procedure should be stopped if:
- Proper instrument application fails
- No descent is achieved with traction
- The fetus is not delivered within a reasonable time frame— after three unsuccessful pulls or if the duration exceeds 15 to 20 minutes.
Sequential Instrument Use
- Sequential use of different instruments (switching from vacuum to forceps or vice versa) is generally discouraged due to increased risks of maternal and neonatal morbidity. This practice should be limited to rare circumstances under the guidance of an experienced clinician.
Post-delivery Examination
After delivery, thorough examinations of the mother and newborn are essential to identify and address any complications resulting from the assisted delivery process.
Newborn Complications:
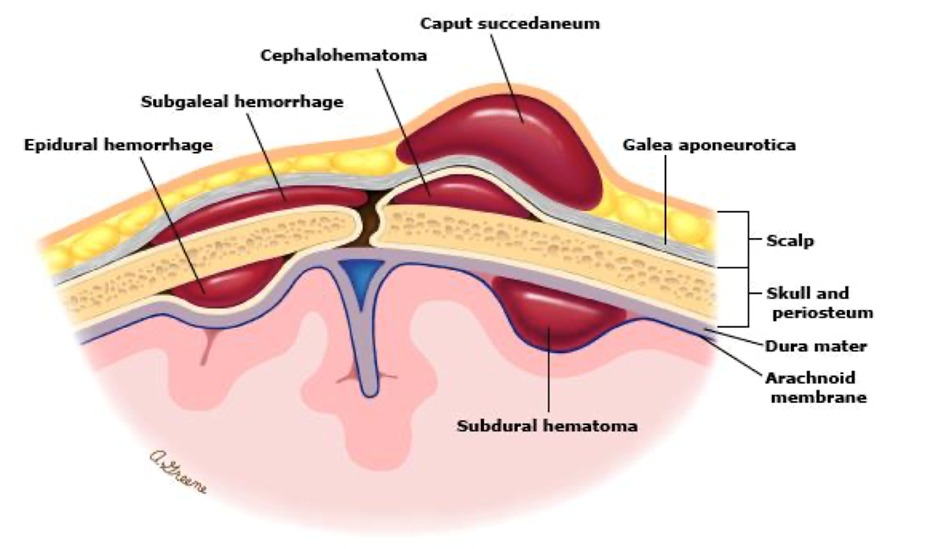
- Intracranial Hemorrhage: Includes epidural, subdural, intraparenchymal, subarachnoid, and intraventricular hemorrhage.
- Subgaleal Hemorrhage: Life-threatening complication particularly associated with vacuum-assisted births.
- Scalp Abrasions and Lacerations: More common with vacuum-assisted births.
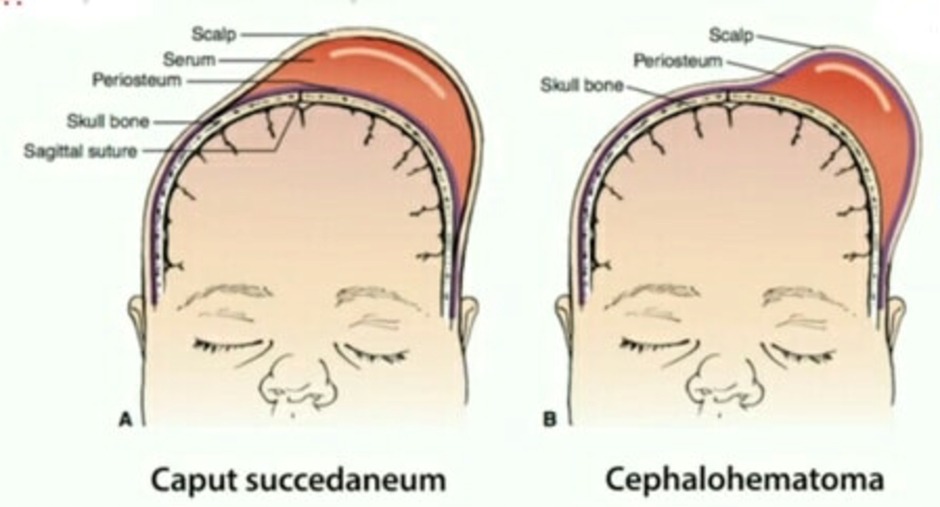
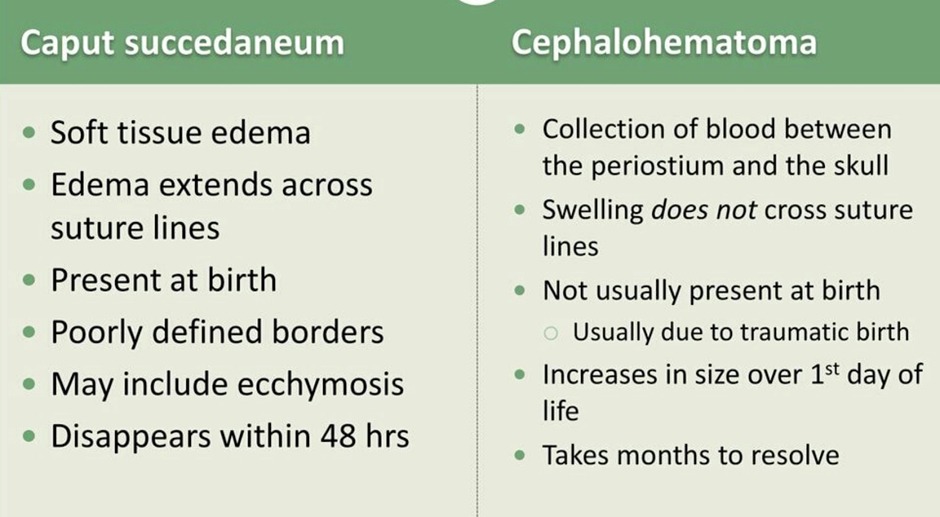
- Cephalohematoma: Occurs more frequently after vacuum-assisted extraction than forceps-assisted birth.
- Retinal Hemorrhage: Higher incidence in vacuum-assisted births, typically resolving without sequelae within four weeks.
- Shoulder Dystocia and Brachial Plexus Injury: More common with vacuum-assisted births.
- Skull Fracture and Facial Nerve Injury: Potential risks with forceps-assisted births.
Maternal Complications:
- Genital Tract Laceration: Including perineal, vulvar, and vaginal trauma.
- Urinary Tract Injury: Bladder and ureteral injuries can occur, especially with forceps-assisted births.
- Anal Sphincter Injury: Occiput posterior position during assisted vaginal birth increases the risk of third-/fourth-degree perineal lacerations.
- Increased Risk of Maternal Morbidity: Sequential use of vacuum and forceps is associated with higher rates of maternal morbidity, including severe perineal lacerations and postpartum hemorrhage.
Conclusion
Assisted vaginal births, employing either forceps or vacuum extraction, remain vital options in modern obstetric care, offering an alternative to cesarean delivery under specific circumstances. These interventions can be lifesaving and pivotal in ensuring the health and safety of both mother and child during the complex process of childbirth. However, the choice to proceed with an assisted delivery is not without its risks and requires a nuanced understanding of the potential complications for both the newborn and the mother.
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.