شرح المدرسين

Summary
A transient ischemic attack (TIA) is a brief episode of focal neurologic dysfunction caused by transient ischemia of the brain, spinal cord, or retina — without acute infarction on imaging. Symptoms are sudden in onset, follow a vascular territory, and typically resolve completely within 1 hour (almost always within 24 hours).
Although the deficit is transient, a TIA is a powerful warning sign of impending stroke and must be treated as a neurologic emergency. Workup centers on identifying the embolic or atherosclerotic source — carotid Doppler, ECG, echocardiography, and neuroimaging — while the ABCD² score helps risk-stratify early stroke recurrence. Cornerstones of secondary prevention are antiplatelet therapy (including short-course dual antiplatelet therapy for high-risk events), high-intensity statins, blood-pressure control, anticoagulation for atrial fibrillation, and carotid endarterectomy for symptomatic high-grade stenosis.
| Important – فكرة سؤال | |
A TIA is a medical emergency, not a benign event. The risk of stroke is highest in the first 48 hours, and up to 10–15% of patients will have a completed stroke within 90 days — half of those within the first 2 days. Urgent evaluation (within 24 hours) is mandatory. |
تذكر |
Definition
A transient ischemic attack is a transient episode of neurologic dysfunction caused by focal brain, spinal cord, or retinal ischemia, without evidence of acute infarction. The defining feature is that ischemia is brief enough that no permanent tissue death occurs.
The definition has shifted from a purely time-based (resolution within 24 hours) to a tissue-based concept, because modern MRI shows that many events lasting under 24 hours have already caused true infarction — and are therefore strokes, not TIAs. Under the current AHA/ASA definition, the distinction between TIA and ischemic stroke rests on whether infarction is present on imaging, not on symptom duration.
| Time-based vs Tissue-based Definition of TIA | ||
|---|---|---|
| Feature | Classic (time-based) | Modern (tissue-based) |
| Definition | Focal neurologic deficit resolving within 24 hours | Transient neurologic dysfunction WITHOUT acute infarction on imaging |
| Basis | Duration of symptoms only | Presence/absence of tissue infarction (MRI-DWI) |
| Problem | Many ‘TIAs’ lasting <24 h actually show infarction on MRI | Reclassifies imaging-positive events as stroke |
| Endorsed by | Older WHO definition | AHA/ASA (current standard) |
Epidemiology
TIA is common and frequently underreported, as transient symptoms are often dismissed by patients. Incidence rises sharply with age and is higher in men, Black populations, and patients with cardiovascular risk factors.
- Incidence: Approximately 200,000–500,000 TIAs are diagnosed annually in the United States; true incidence is higher because many are never reported.
- Age: Risk increases markedly after age 60; most patients are elderly.
- Stroke risk: About 1 in 3 patients with an untreated TIA will eventually have a stroke, and roughly 10–15% within 90 days — the majority within the first 2 days.
- Preceding stroke: Up to 15–30% of ischemic strokes are preceded by a TIA, making it a critical and treatable warning event.
Etiology
A TIA shares the same etiological spectrum as ischemic stroke — the only difference is that ischemia is brief enough to avoid infarction. Establishing the underlying mechanism is the entire purpose of the workup, because each cause has a distinct secondary-prevention strategy. See the comparison of ischemic and hemorrhagic stroke subtypes for how thrombotic, embolic, and hemorrhagic mechanisms differ.
| Etiology of TIA (same mechanisms as ischemic stroke): Identifying the mechanism drives secondary prevention | |
| Large-vessel | Atherothromboembolism |
| Carotid / vertebral atherosclerosis | Artery-to-artery embolism from a plaque; symptomatic carotid stenosis is the key surgically treatable cause |
| Aortic arch atheroma | Proximal embolic source |
| Cardioembolic | Heart as embolic source |
| Atrial fibrillation | Most common cardioembolic cause; mandates anticoagulation |
| Valvular / prosthetic valve, recent MI, LV thrombus, endocarditis | Mural or valvular thrombus embolizes to brain |
| Patent foramen ovale | Paradoxical embolism, especially in younger patients |
| Small-vessel | Lipohyalinosis |
| Lacunar mechanism | Hypertension/diabetes-driven small penetrating artery disease; pure motor or pure sensory transient deficits |
| Other | Less common |
| Hypercoagulable states, vasculitis, arterial dissection | Consider in young patients without vascular risk factors |
| Hypoperfusion (e.g., subclavian steal) | Watershed/posterior symptoms from flow reversal or low flow |
Risk factors mirror those of atherosclerosis and cardioembolism: hypertension (the single most important modifiable factor), diabetes, dyslipidemia, smoking, atrial fibrillation, older age, prior stroke/TIA, and carotid disease.
Pathophysiology
TIA results from temporary, reversible hypoperfusion of a focal region of CNS or retinal tissue. Because flow is restored before metabolic failure causes cell death, the deficit resolves and no infarct forms. Two principal mechanisms operate:
- Embolic (most common): An embolus from a carotid plaque, the aortic arch, or the heart lodges in a cerebral or retinal artery, then fragments or passes distally, restoring perfusion and aborting the deficit. Most clinically meaningful TIAs are micro-embolic.
- Hemodynamic / hypoperfusion: A fixed high-grade stenosis plus a transient drop in perfusion pressure (e.g., postural change, arrhythmia, flow reversal) produces border-zone ischemia that reverses when flow normalizes.
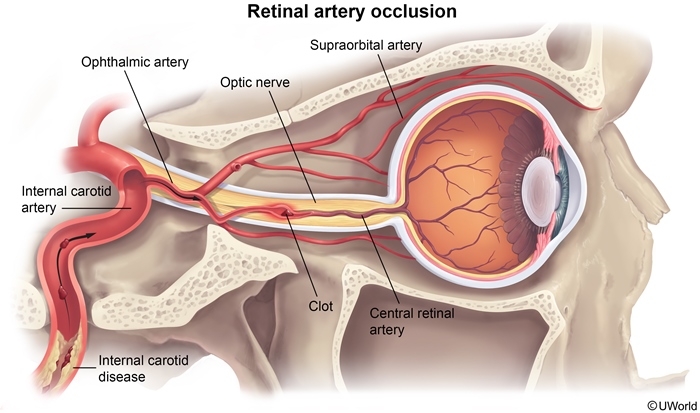
When the embolus travels via the internal carotid → ophthalmic → central retinal artery, the patient experiences amaurosis fugax: a transient, painless, monocular "curtain" descending over vision. This is effectively a TIA of the retina and a strong marker of ipsilateral carotid disease.
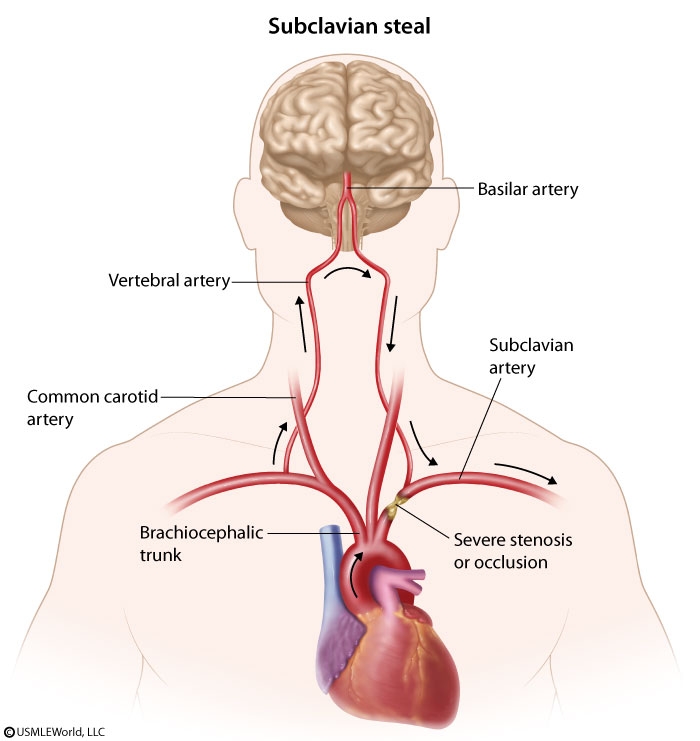
Posterior-circulation TIAs can also arise from subclavian steal: proximal subclavian artery stenosis causes retrograde (reversed) flow down the ipsilateral vertebral artery, "stealing" blood from the basilar system during arm exertion. Clues are a blood-pressure difference between arms and a supraclavicular bruit, with symptoms of vertebrobasilar insufficiency (vertigo, ataxia, diplopia).
Clinical Features
TIA symptoms are sudden in onset, focal, maximal at onset, and "negative" (loss of function), reflecting the vascular territory involved. They resolve completely, usually within minutes to an hour. The localization (carotid vs vertebrobasilar) points toward the likely embolic source and guides imaging.
| Localizing TIA by Vascular Territory | ||
|---|---|---|
| Feature | Carotid (anterior circulation) | Vertebrobasilar (posterior circulation) |
| Vision | Amaurosis fugax (transient monocular blindness) | Homonymous hemianopia, diplopia |
| Motor/sensory | Unilateral weakness or numbness (face/arm/leg) | Bilateral or alternating weakness/numbness |
| Speech | Aphasia (dominant hemisphere) | Dysarthria |
| Coordination/balance | Usually spared | Vertigo, ataxia, gait imbalance |
| Other clues | Carotid bruit | Drop attacks, crossed signs, bilateral symptoms |
| Note – ملاحظة | |
Features that argue against a TIA and suggest a mimic include: gradual march of symptoms over minutes (migraine aura), positive phenomena such as flashing lights or rhythmic jerking (seizure/migraine), and isolated symptoms — vertigo, dizziness, syncope, or amnesia alone are rarely a TIA. TIA deficits are sudden, maximal at onset, focal, and 'negative' (loss of function). |
ملاحظة |
Diagnosis
TIA is a clinical diagnosis — by the time the patient is assessed, the deficit has usually resolved and the neurologic exam is normal. The goals of investigation are to (1) confirm an ischemic mechanism and exclude mimics, (2) identify the embolic/atherosclerotic source, and (3) risk-stratify early recurrence. Workup should be urgent (within 24 hours of a recent event).
Neuroimaging: MRI with diffusion-weighted imaging (DWI) is the preferred study — it confirms there is no acute infarction (which would reclassify the event as stroke) and detects clinically silent lesions. Non-contrast CT head is obtained early to exclude hemorrhage and structural mimics, especially before antithrombotic therapy.
Vascular imaging: Carotid Doppler ultrasonography is the first-line screening test for carotid stenosis in anterior-circulation events; CT angiography or MR angiography confirms the degree of stenosis and assesses intracranial and vertebrobasilar vessels.
Cardiac evaluation: 12-lead ECG (and prolonged/Holter or extended monitoring) to detect atrial fibrillation; echocardiography (transthoracic ± transesophageal) to identify an intracardiac thrombus, valvular source, or patent foramen ovale.
Serum / laboratory: Capillary/serum glucose (hypoglycemia is a key TIA mimic), CBC, electrolytes, renal function, fasting lipids, HbA1c, and coagulation studies. Consider ESR/CRP and a hypercoagulable workup in young patients without conventional risk factors.
| Important – فكرة سؤال | |
Every TIA patient needs a search for a cardioembolic source: ECG (for atrial fibrillation), prolonged rhythm monitoring, and echocardiography. In a patient with a prosthetic (e.g., bioprosthetic mitral) valve and a new TIA, suspect prosthetic valve thrombosis — the next best step is echocardiography, not simply starting an antiplatelet. |
تذكر |
Risk stratification — ABCD² score: Estimates short-term stroke risk after a TIA and guides urgency of admission and intervention. Points are assigned for:
- Age ≥ 60 years — 1 point
- Blood pressure ≥ 140/90 mmHg — 1 point
- Clinical features — unilateral weakness (2) or speech disturbance without weakness (1)
- Duration — ≥ 60 min (2) or 10–59 min (1)
- Diabetes — 1 point
The total ranges 0–7; higher scores predict greater 2-, 7-, and 90-day stroke risk, and a score ≥ 4 generally favors hospital admission and expedited workup. Refer to the ABCD² score risk-stratification table for the stratified stroke-risk percentages at each cut-off.
Differential Diagnosis
Because the deficit has typically resolved by presentation, the differential rests on the history. The first priority is to separate TIA from ischemic stroke (deficit persists / infarct on DWI) and from intracerebral hemorrhage (excluded on CT before antithrombotics). The remaining mimics produce transient neurologic symptoms but differ in tempo and character.
| Differential Diagnosis of TIA (“TIA mimics”): How to distinguish each from a true TIA | |
| Vascular | Must exclude first |
| Ischemic stroke | Identical onset but deficit persists / infarction on DWI-MRI |
| Intracerebral hemorrhage | Headache, depressed consciousness; blood on CT |
| Neurologic | Episodic disorders |
| Seizure / Todd paralysis | Positive phenomena (jerking), post-ictal deficit resolving over hours, tongue biting |
| Migraine with aura | Gradual march over minutes, positive visual phenomena (scintillations), headache follows, younger patients |
| Transient global amnesia | Isolated anterograde amnesia, repetitive questioning, no focal deficit |
| Metabolic / Systemic | Reversible mimics |
| Hypoglycemia | Focal deficit possible; resolves with glucose — always check a fingerstick |
| Syncope / pre-syncope | Global hypoperfusion, loss of consciousness, no focal signs |
| Other | Peripheral / functional |
| Bell palsy / peripheral vertigo (BPPV, vestibular neuritis) | Peripheral pattern; isolated vertigo is rarely a TIA |
| Functional / conversion | Non-anatomic distribution, inconsistent exam |
Management
Management of TIA is secondary stroke prevention started immediately. Two arms run in parallel: (1) antithrombotic therapy plus aggressive risk-factor control for all patients, and (2) source-specific therapy — anticoagulation for atrial fibrillation, and carotid revascularization for symptomatic high-grade stenosis. The full menu of agents is summarised in the antiplatelet and antithrombotic options for ischemic stroke/TIA.
Acute approach
- Step 1 — Stabilize and image: Check glucose, obtain non-contrast CT to exclude hemorrhage, and risk-stratify with the ABCD² score. Admit/observe high-risk patients (ABCD² ≥ 4, crescendo TIAs, or known high-grade carotid stenosis).
- Step 2 — Start antiplatelet therapy promptly: For most TIAs, aspirin 162–325 mg load then 75–100 mg PO daily. For high-risk TIA (ABCD² ≥ 4) or minor stroke, give short-course dual antiplatelet therapy (DAPT) within 24 hours — clopidogrel 300–600 mg load + aspirin, then aspirin 81 mg + clopidogrel 75 mg daily for 21 days, then step down to a single agent. Prolonged DAPT increases bleeding without added benefit.
- Step 3 — Treat a cardioembolic source: If atrial fibrillation is found, use anticoagulation (a DOAC, or warfarin for mechanical valves/mitral stenosis) rather than antiplatelet therapy.
- Step 4 — Refer for carotid revascularization when symptomatic high-grade stenosis is present (see below), ideally within 2 weeks of the event.
| Antiplatelet Regimens for Secondary Prevention after TIA | ||
|---|---|---|
| Regimen | Dose | When used |
| Aspirin (monotherapy) | 162–325 mg load, then 75–100 mg PO daily | Default long-term antiplatelet for non-cardioembolic TIA |
| Clopidogrel (monotherapy) | 75 mg PO daily | Alternative single agent; aspirin intolerance/allergy |
| DAPT (aspirin + clopidogrel) | Clopidogrel 300–600 mg load + aspirin, then aspirin 81 mg + clopidogrel 75 mg daily × 21 days → then single agent | High-risk TIA (ABCD² ≥ 4) or minor stroke, started within 24 h |
| Aspirin + ER dipyridamole | 25 mg / 200 mg PO twice daily | Alternative long-term option |
Risk-factor modification (all patients)
- High-intensity statin: e.g., atorvastatin 80 mg PO daily — indicated for all TIA/ischemic-stroke patients as ASCVD secondary prevention regardless of baseline LDL. The statin indications for ASCVD prevention lists prior TIA/stroke as a class I indication.
- Blood-pressure control: the single most important modifiable risk factor; target per guidelines after the acute phase.
- Anticoagulation for AF: guided by the CHA₂DS₂-VASc score; a prior TIA already contributes 2 points, so virtually all such patients qualify for anticoagulation.
- Glycemic control, smoking cessation, weight loss, and exercise.
Carotid revascularization
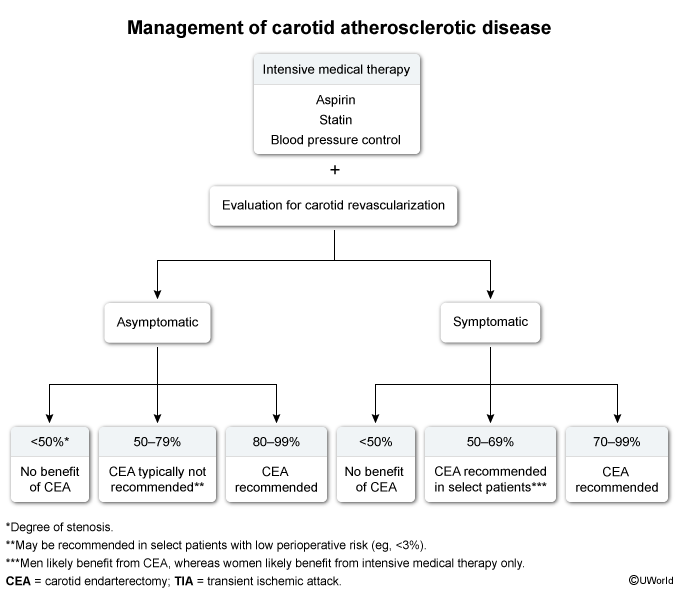
For symptomatic carotid stenosis (deficits in the territory of the affected artery within the prior 6 months), the degree of stenosis drives the decision:
- 70–99% stenosis: carotid endarterectomy (CEA) is generally recommended (plus intensive medical therapy).
- 50–69% stenosis: CEA is beneficial mainly in men; medical management alone is favored in women.
- < 50% stenosis: no proven benefit from revascularization — medical therapy only.
Carotid artery stenting is an alternative in selected patients but carries a higher periprocedural (30-day) stroke/death risk. A near-total occlusion (≈100%) is generally not revascularized.
Complications & Prognosis
The dominant complication of TIA is a subsequent ischemic stroke. Risk is front-loaded: roughly half of post-TIA strokes occur within the first 48 hours, which is why evaluation and treatment are urgent. These patients also share systemic atherosclerotic risk and are prone to myocardial infarction and vascular death.
- Early stroke risk: ≈10–15% at 90 days untreated; the ABCD² score stratifies 2-, 7-, and 90-day risk (higher scores = higher risk).
- Recurrent TIA / crescendo TIAs: increasingly frequent events signal an unstable source (often high-grade carotid stenosis) and herald imminent stroke.
- Cardiovascular morbidity: elevated long-term risk of MI and cardiovascular death.
Prognosis improves markedly with prompt, guideline-based secondary prevention — urgent antithrombotic therapy, statins, blood-pressure and AF management, and timely carotid revascularization can reduce subsequent stroke risk by roughly 80%. Conversely, untreated patients face a substantial lifetime stroke burden, with about one-third eventually suffering a stroke.
Mnemonics
| Mnemonic – جملة تذكرية | |
ABCD² — early stroke-risk score after TIA:
FAST — recognize the deficit & act: Face droop, Arm weakness, Speech difficulty, Time to call for help. |
جملة تذكرية |
Carotid surgery rule of thumb — for symptomatic stenosis: "70 = operate" (CEA for 70–99%), "50 = it depends" (benefit mainly in men for 50–69%), "under 50 = medicate" (medical therapy only for < 50%).
Key Points for Exams – نقاط مهمة للامتحانات
- Definition: transient focal neurologic dysfunction from ischemia without infarction on imaging — the modern tissue-based definition replaces the old <24-hour rule.
- TIA = neurologic emergency: ~half of post-TIA strokes occur within 48 hours; evaluate within 24 hours.
- Amaurosis fugax = transient painless monocular vision loss ("curtain") → think ipsilateral carotid disease.
- Anterior (carotid) = amaurosis fugax, unilateral weakness, aphasia; posterior (vertebrobasilar) = vertigo, ataxia, diplopia, bilateral/crossed signs.
- Always check glucose — hypoglycemia is a classic mimic. MRI-DWI confirms no infarct; CT excludes hemorrhage.
- Find the source: carotid Doppler (first-line vascular test), ECG + monitoring for AF, and echocardiography.
- ABCD² stratifies early stroke risk; score ≥ 4 → admit/expedite workup.
- Antithrombotics: aspirin for most; DAPT (aspirin + clopidogrel) × 21 days for high-risk TIA/minor stroke; anticoagulate if AF.
- All patients: high-intensity statin (atorvastatin 80 mg) regardless of LDL, BP control, smoking cessation.
- Carotid endarterectomy for symptomatic 70–99% stenosis; 50–69% benefits men; < 50% medical therapy only.
- Prosthetic valve + new TIA → suspect prosthetic valve thrombosis → next step is echocardiography.
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.