شرح المدرسين

Summary
Cerebrovascular circulation divides into the anterior (ICA: supplying ACA and MCA) and posterior (vertebrobasilar: supplying PCA and brainstem) systems, joined at the base of the brain by the Circle of Willis. Vascular occlusions produce territory-specific neuro deficits: ACA strokes cause contralateral leg weakness and urinary incontinence, MCA strokes produce contralateral face/arm weakness with aphasia (dominant) or hemineglect (non-dominant), and PCA strokes cause contralateral homonymous hemianopia with macular sparing. Perforating lenticulostriate end-arteries are vulnerable to lipohyalinosis, causing pure motor lacunar infarcts or deep intracerebral hemorrhages (most common in the putamen). Saccular (berry) aneurysms occur at arterial bifurcations; ACom is the most common site, while PCom aneurysms present with painful, pupil-involving CN III palsy. Non-contrast head CT is the first-line diagnostic test to exclude hemorrhage before initiating thrombolysis.
Overview – نظرة عامة
The brain is ~2% of body weight yet receives roughly 15–20% of resting cardiac output and consumes ~20% of total oxygen and glucose. Because neurons store almost no energy substrate, interruption of flow for only minutes causes infarction — this is why cerebrovascular anatomy is one of the highest-yield localisation tools in clinical neurology.
Blood reaches the brain through two paired arterial systems: the internal carotid arteries (ICA), supplying the anterior circulation, and the vertebral arteries, supplying the posterior (vertebrobasilar) circulation. Inferiorly these two systems are joined by the Circle of Willis, an anastomotic ring that provides collateral flow when one inflow vessel is compromised. Three paired surface arteries — the anterior (ACA), middle (MCA), and posterior cerebral arteries (PCA) — perfuse discrete cortical territories whose somatotopic (homunculus) organisation lets you predict the deficit produced by each occlusion.
Proximal arterial supply: from the aortic arch to the skull base
Knowing the proximal pathway explains why emboli of cardiac or aortic origin preferentially reach certain territories.
Aortic arch branches (left to right): the brachiocephalic (innominate) trunk → right common carotid + right subclavian; the left common carotid; and the left subclavian. The right vertebral arises from the right subclavian, the left vertebral from the left subclavian.
Carotid system: each common carotid bifurcates at the upper border of the thyroid cartilage (~C3–C4) into the external carotid (face/scalp) and the internal carotid (brain). The ICA ascends without branching in the neck, then passes through the petrous bone and cavernous sinus. Its intracranial branches, in order, are the ophthalmic artery → posterior communicating artery (PCom) → anterior choroidal artery, before it terminates by dividing into the ACA and MCA.
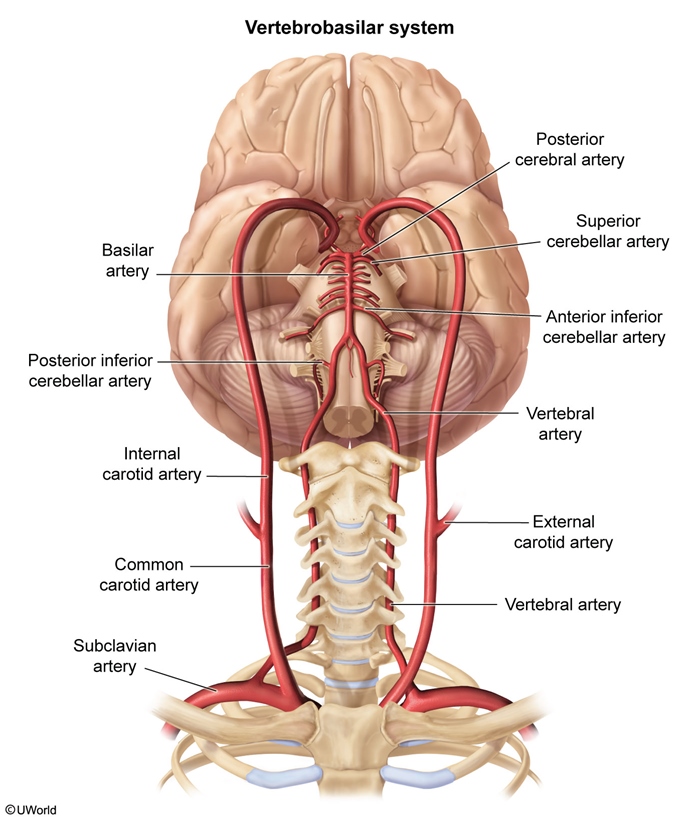
Vertebrobasilar system: the paired vertebral arteries ascend through the transverse foramina of C6–C1, pierce the dura at the foramen magnum, give off the posterior inferior cerebellar artery (PICA) and the anterior spinal artery, then fuse at the pontomedullary junction to form the single basilar artery.
| Important – فكرة سؤال | |
|
The ophthalmic artery is the first major intracranial branch of the ICA. An embolus from carotid atherosclerosis lodging here produces amaurosis fugax — transient, painless, monocular visual loss classically described as a 'curtain descending' over one eye. This is an ipsilateral warning sign of internal carotid stenosis and a TIA-equivalent that warrants carotid imaging. |
تذكر |
The Circle of Willis: the anastomotic ring
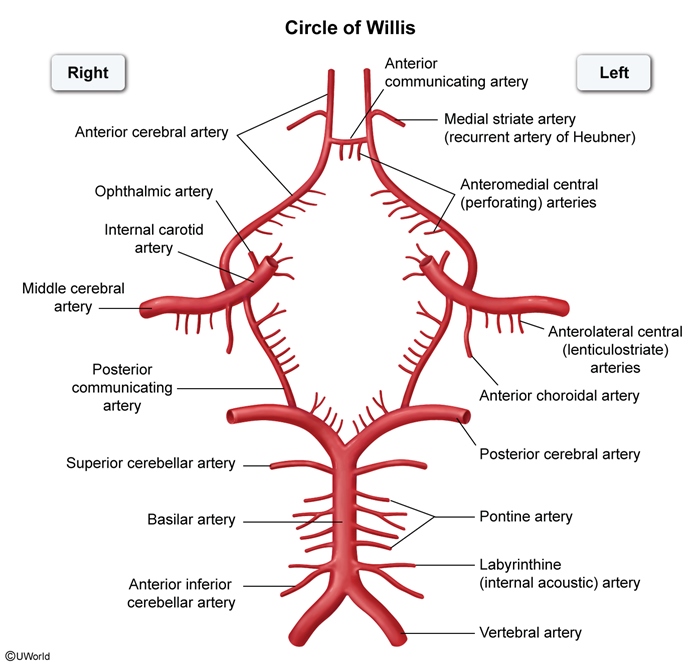
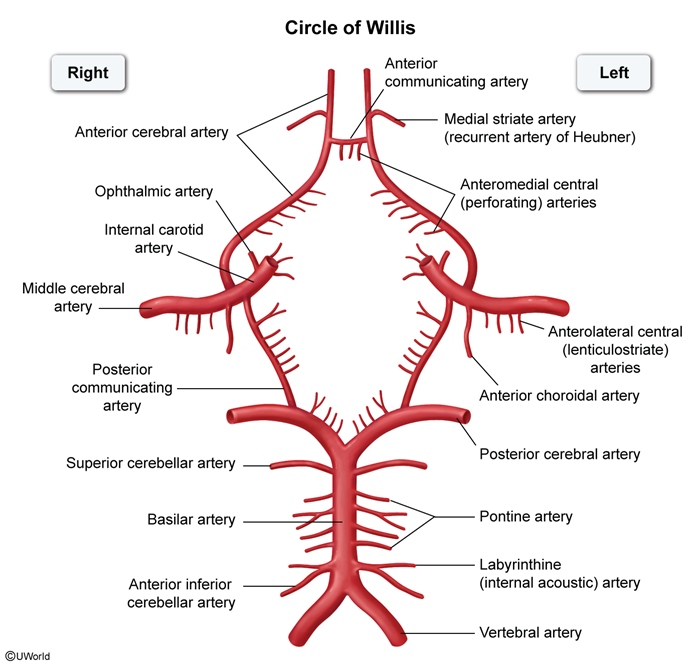
The Circle of Willis is a heptagonal arterial ring at the base of the brain that unites the anterior and posterior circulations and the right and left hemispheres. Its purpose is collateral perfusion: if one inflow vessel is gradually occluded, flow can be recruited across the communicating arteries to protect the downstream territory. Sudden occlusion, however, often outpaces collateral recruitment and still causes infarction.
Tracing the ring: the two ACAs are joined anteriorly by the single anterior communicating artery (ACom); each ICA contributes the proximal ACA and MCA; each PCom connects the ICA to the ipsilateral PCA; and the two PCAs arise from the bifurcation of the basilar artery posteriorly.
A complete, symmetric circle is present in only ~20–50% of people; anatomic variants (hypoplastic or absent communicating segments, a fetal-origin PCA arising from the ICA rather than the basilar) are common and clinically important because they reduce collateral reserve.
| Anterior vs Posterior Circulation | ||
|---|---|---|
| Feature | Anterior circulation | Posterior circulation |
| Inflow vessels | Internal carotid arteries | Vertebral → basilar artery |
| Surface arteries | ACA, MCA | PCA (+ cerebellar arteries: PICA, AICA, SCA) |
| Connected to ring by | Anterior communicating artery (ACom) | Posterior communicating arteries (PCom) |
| Main territory | Frontal, parietal, lateral temporal lobes; deep grey matter | Occipital lobe, medial temporal lobe, brainstem, cerebellum, thalamus |
| Classic deficits | Hemiparesis, aphasia, neglect, gaze deviation | Visual field loss, crossed brainstem syndromes, vertigo/ataxia, coma |
| Mnemonic – جملة تذكرية | |
|
The Circle of Willis has 9 arteries forming the ring — count them as '2-2-2-2-1': 2 ACA, 2 ICA (terminal segments), 2 PCom, 2 PCA, and 1 ACom. Rule of thumb: communicating arteries connect; cerebral arteries supply. A single ACom bridges the front, paired PComs bridge front-to-back on each side. |
جملة تذكرية |
Anterior circulation: ICA, ACA and MCA territories
The ICA terminates as the ACA and MCA, which together perfuse most of the cerebral convexity and the deep grey matter of each hemisphere.
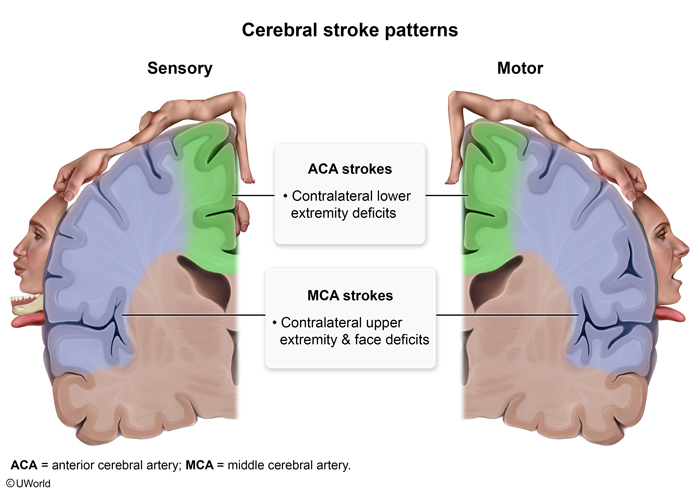
The anterior cerebral artery (ACA) curves over the corpus callosum to supply the medial surface of the frontal and parietal lobes — the cortex that contains the leg and foot region of the motor/sensory homunculus and the frontal micturition centre.
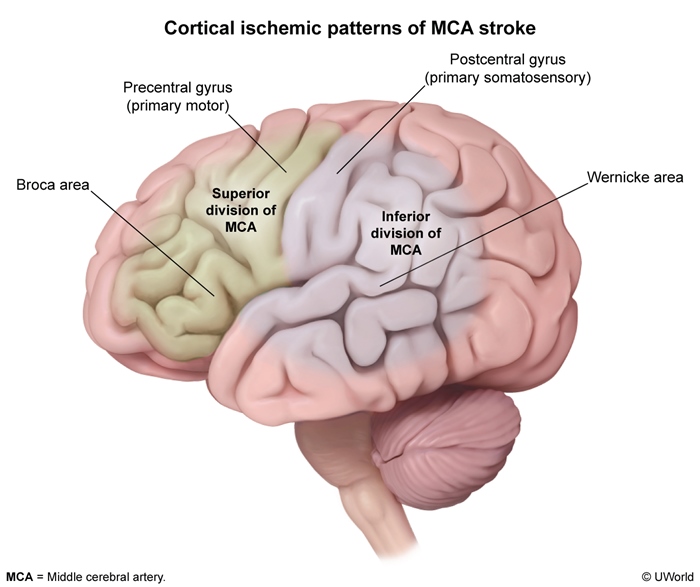
The middle cerebral artery (MCA) is the direct continuation of the ICA and the most common site of embolic stroke. It fans across the lateral hemisphere, supplying the face/arm homunculus, Broca and Wernicke language areas in the dominant hemisphere, and (via deep lenticulostriate branches) the basal ganglia and internal capsule. The MCA splits into a superior division (frontal cortex, Broca area → expressive aphasia) and an inferior division (temporoparietal cortex, Wernicke area → receptive aphasia).
| ACA vs MCA — Territory and Deficits | ||
|---|---|---|
| Feature | Anterior cerebral artery (ACA) | Middle cerebral artery (MCA) |
| Cortical territory | Medial frontal & parietal lobes (interhemispheric surface) | Lateral surface of the hemisphere (most of frontal, parietal, temporal) |
| Homunculus region | Leg / foot area (medial) | Face, hand, arm area (lateral) |
| Motor/sensory deficit | Contralateral LEG > arm weakness & sensory loss | Contralateral FACE/ARM > leg weakness & sensory loss |
| Higher cortical signs | Abulia, frontal release signs, urinary incontinence (micturition center) | Aphasia (dominant), neglect (non-dominant), gaze deviation toward lesion |
| Visual | — | Contralateral homonymous hemianopia (optic radiations) |
For a consolidated map of deficits by occluded vessel, see the clinical deficits of major cerebrovascular occlusions, which links each artery to its signature syndrome.
| Important – فكرة سؤال | |
|
ACA = leg, MCA = face/arm. A patient with isolated contralateral lower-limb upper-motor-neuron weakness (often with urinary incontinence) has an ACA infarct — the leg/foot homunculus sits on the medial cortex the ACA supplies. Note that an embolus distal to the ACom is NOT rescued by collateral flow, so a unilateral ACA stroke still produces a unilateral leg deficit. By contrast, MCA strokes spare the leg relatively and hit the face/arm plus language or neglect. |
تذكر |
Posterior circulation: the vertebrobasilar system
The vertebrobasilar system supplies the brainstem, cerebellum, thalamus, occipital lobe and medial temporal lobe. Because the brainstem packs cranial-nerve nuclei alongside ascending/descending long tracts, its strokes characteristically produce "crossed" syndromes — ipsilateral cranial-nerve signs with contralateral body weakness/sensory loss.
From the vertebral arteries upward:
- PICA (off the vertebral) → lateral medulla and inferior cerebellum.
- Basilar artery → gives AICA (lateral pons, plus the labyrinthine artery to the inner ear), numerous pontine perforators (basis pontis), and SCA (superior cerebellum), before bifurcating into the two PCAs.
- PCA → occipital lobe (primary visual cortex), inferomedial temporal lobe, and (via thalamoperforators) the thalamus.
Two named syndromes recur on exams: lateral medullary (Wallenberg) syndrome from PICA/vertebral occlusion (ipsilateral facial sensory loss, Horner syndrome, dysphagia/hoarseness, vertigo, ataxia; contralateral body pain/temperature loss) and Weber syndrome from a midbrain PCA-branch occlusion (ipsilateral CN III palsy + contralateral hemiparesis). The full set is laid out in the posterior circulation stroke syndromes, contrasting Weber, Wallenberg, medial medullary and cerebellar strokes.
| Mnemonic – جملة تذكرية | |
|
Cerebellar arteries from bottom to top spell 'PICA → AICA → SCA'. Lateral brainstem syndromes: PICA = lateral medulla = Wallenberg; AICA = lateral pons = facial palsy + deafness (the 'Facial droop means AICA's pooped' rule, because AICA also feeds the labyrinthine artery to the inner ear). Pin it down: PICA → swallowing (medulla), AICA → hearing/face (pons). |
جملة تذكرية |
| Important – فكرة سؤال | |
|
PCA occlusion → contralateral homonymous hemianopia WITH macular sparing. The occipital pole (macular/central vision) receives collateral supply from MCA branches, so central vision is preserved despite loss of the peripheral field. Macular sparing is the classic clue that an occipital (PCA) infarct — not an optic-tract or radiation lesion — is responsible. |
تذكر |
Deep penetrating (perforating) arteries
Beyond the surface arteries, small perforating (penetrating) arteries dive into the brain to supply the deep grey matter and white-matter tracts. They are end arteries — sparsely anastomotic — which makes their territories vulnerable to discrete lacunar infarcts and to hypertensive hemorrhage.
| Perforating artery | Origin | Territory supplied | Classic lacunar syndrome |
|---|---|---|---|
| Lenticulostriate | MCA (M1 segment) | Putamen, globus pallidus, internal capsule, caudate | Pure motor hemiparesis; #1 site of hypertensive ICH |
| Anterior choroidal | ICA (before bifurcation) | Posterior limb of internal capsule, optic tract, lateral geniculate | Hemiparesis + hemisensory loss + homonymous hemianopia |
| Recurrent artery of Heubner | Proximal ACA (A1–A2) | Anterior limb of internal capsule, head of caudate | Face/arm weakness, dysarthria |
| Thalamoperforators | PCA / PCom (P1) | Thalamus | Pure sensory stroke |
| Pontine perforators | Basilar artery | Basis pontis | Dysarthria–clumsy hand; ataxic hemiparesis |
For the localisation of each small-vessel pattern, refer to the lacunar stroke syndromes and their anatomical sites, which maps pure motor, pure sensory, ataxic-hemiparesis and dysarthria–clumsy-hand patterns to the internal capsule, thalamus and basis pontis.
| Important – فكرة سؤال | |
|
The deep perforators are end (terminal) arteries with no collateral supply. Chronic hypertension drives lipohyalinosis and Charcot–Bouchard microaneurysms in these vessels, producing two opposite lesions: occlusion → lacunar (small-vessel) infarcts, and rupture → deep hypertensive intracerebral hemorrhage (most often in the putamen/basal ganglia via lenticulostriate vessels). A pure motor lacunar stroke localises to the posterior limb of the internal capsule or basis pontis — with no cortical signs (no aphasia, neglect, or visual loss). |
تذكر |
Cortical vascular territories and the homunculus
The cerebral cortex is mapped into three non-overlapping arterial territories, and superimposing the motor/sensory homunculus on this map turns "which artery?" into "which body part and which higher function?".
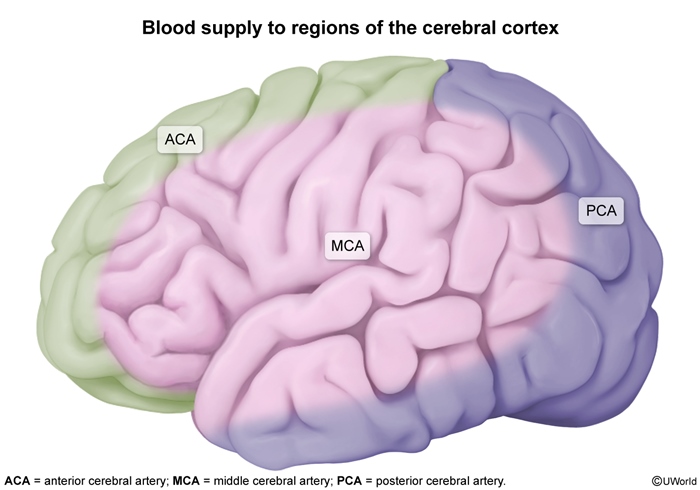
The homunculus runs medially-to-laterally along the precentral (motor) and postcentral (sensory) gyri: the foot and leg hang over the medial interhemispheric surface (ACA), while the trunk, arm, hand and face occupy the lateral convexity (MCA). The hand and face have disproportionately large cortical representation, so MCA strokes produce prominent hand and facial weakness.
Language and spatial attention are also territory-bound: Broca (inferior frontal) and Wernicke (superior temporal) areas lie in the dominant-hemisphere MCA territory, whereas the non-dominant MCA parietal cortex governs spatial attention. The primary visual cortex sits in the occipital lobe within the PCA territory.
| Note – ملاحظة | |
|
One-line localisation shortcut: medial cortex = ACA = leg; lateral cortex = MCA = face/arm + language; occipital cortex = PCA = vision. Add hemisphere dominance: a left (dominant) MCA stroke gives aphasia; a right (non-dominant) MCA stroke gives hemineglect and anosognosia. |
ملاحظة |
Watershed (border-zone) areas
Watershed (border) zones are the thin regions where the distal-most twigs of two adjacent arterial territories meet. They are the last fields to be perfused and therefore the first to infarct when cerebral perfusion pressure falls globally.
Two cortical border zones matter most: the ACA–MCA zone (a parasagittal strip over the frontoparietal convexity) and the MCA–PCA zone (parieto-occipital). A deeper internal (subcortical) watershed lies in the white matter between the deep perforators and the superficial MCA branches.

| Important – فكرة سؤال | |
Watershed infarcts follow global hypoperfusion (cardiac arrest, severe hypotension/sepsis, critical carotid stenosis) rather than a single-vessel embolus. The cortical ACA–MCA border zone sits over the proximal arm and leg homunculus → 'man-in-a-barrel' syndrome: bilateral proximal arm and thigh weakness with preserved distal hands and feet. The MCA–PCA border zone produces higher-order visual deficits. Look for a precipitating hypotensive event in the stem. |
تذكر |
Cerebral venous drainage
Venous blood drains in two tiers. Superficial cortical veins and deep veins (internal cerebral veins → great vein of Galen) empty into the dural venous sinuses — valveless channels between the periosteal and meningeal dura. Flow runs superior sagittal → confluence of sinuses → transverse → sigmoid → internal jugular vein. The cavernous sinuses drain anteriorly and communicate posteriorly via the petrosal sinuses.
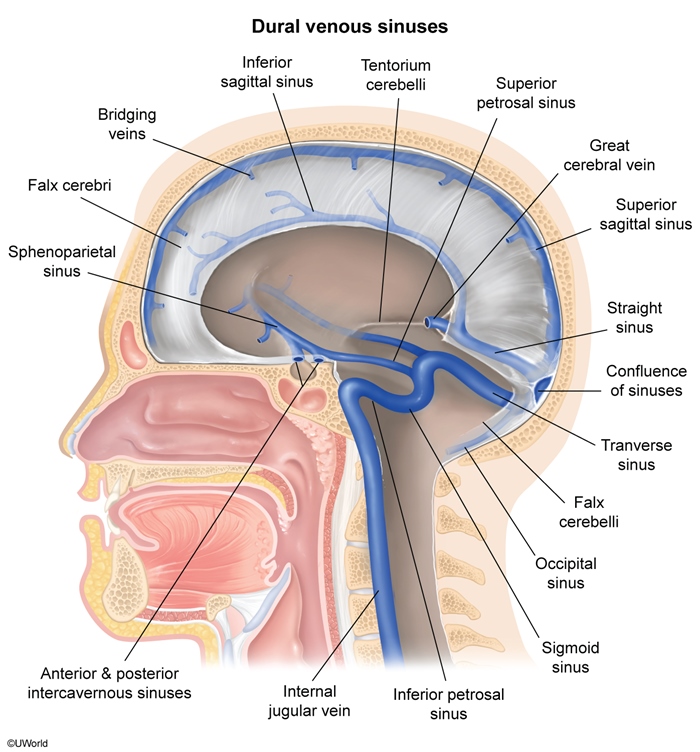
Clinically: torn bridging veins cause subdural hematoma; the superior sagittal sinus resorbs CSF at the arachnoid granulations, so cerebral venous sinus thrombosis can raise intracranial pressure and cause venous (often hemorrhagic) infarcts that do not respect arterial territories.
| Note – ملاحظة | |
The cavernous sinus transmits CN III, IV, V1, V2, and VI plus the cavernous ICA. CN VI runs free within the sinus (next to the ICA), so it is the first nerve affected in cavernous sinus pathology. Cavernous sinus thrombosis (often from facial/sphenoid infection) presents with painful ophthalmoplegia, proptosis and chemosis. |
ملاحظة |
Clinical correlations: aneurysms, hemorrhage and herniation
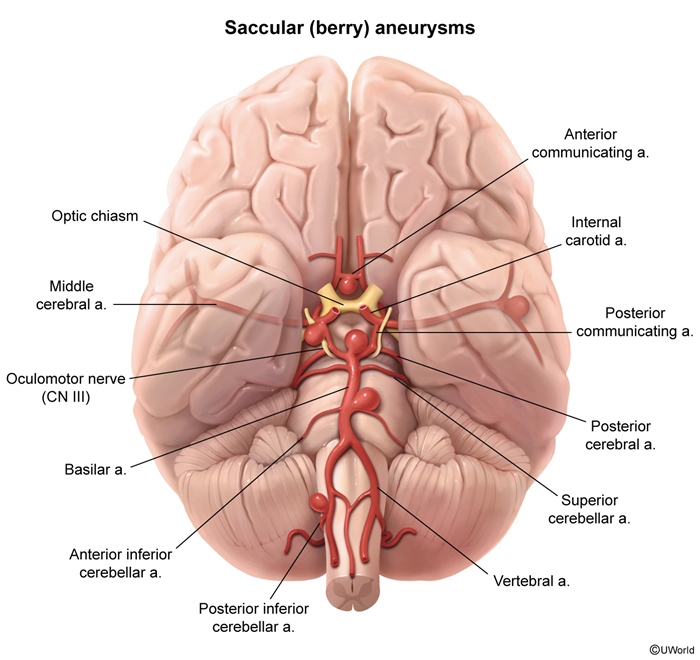
Saccular ("berry") aneurysms form at arterial bifurcations of the Circle of Willis, where wall stress is highest and the media is congenitally thin. In descending frequency they cluster at the anterior communicating artery (~30–35%, the single most common site), the PCom–ICA junction, and the MCA bifurcation. Rupture causes subarachnoid hemorrhage — a thunderclap "worst headache of life."
Location predicts the syndrome. An ACom aneurysm can compress the optic chiasm from above (bitemporal field changes) and, when it ruptures, classically causes SAH with frontal/leg signs. A PCom aneurysm compresses the adjacent oculomotor nerve.
Deep hypertensive hemorrhage (from lenticulostriate Charcot–Bouchard aneurysms) targets the putamen, thalamus, pons and cerebellum. To place these alongside ischemic mechanisms, compare the thrombotic, embolic, intracerebral and subarachnoid stroke subtypes and their distinguishing features.
| Important – فكرة سؤال | |
|
PCom aneurysm → CN III palsy with a 'down-and-out' eye, ptosis, and a fixed dilated pupil. Pupillary fibres travel on the outer surface of CN III, so a compressive lesion (aneurysm, uncal herniation) blows the pupil early — unlike an ischemic (diabetic) CN III palsy, which classically spares the pupil. A painful, pupil-involving third-nerve palsy is a posterior communicating artery aneurysm until proven otherwise and is a neurosurgical emergency. |
تذكر |
| Note – ملاحظة | |
|
Herniation compresses arteries against dural edges: subfalcine (cingulate) herniation compresses the ACA → contralateral leg weakness; uncal (transtentorial) herniation compresses CN III (blown pupil) and the PCA → occipital infarct with contralateral hemianopia. |
ملاحظة |
Imaging anatomy of the cerebral vessels
Several modalities visualise this anatomy in the living patient:
- Non-contrast CT (first-line in acute stroke): rapidly excludes hemorrhage before thrombolysis; SAH appears as blood in the basal cisterns.
- CT angiography (CTA): fast, widely available; identifies large-vessel occlusion and aneurysms for thrombectomy/clipping decisions.
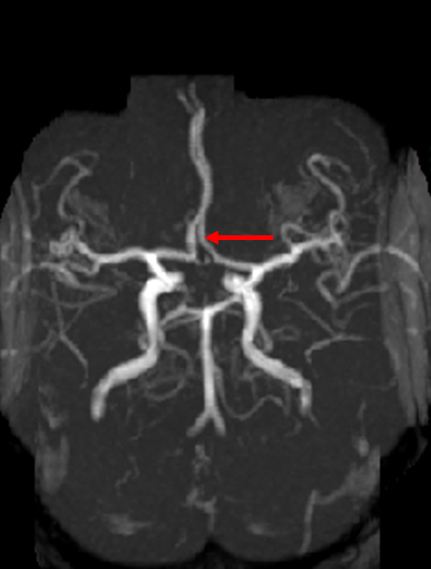
- MR angiography (MRA): time-of-flight technique images the Circle of Willis without contrast; excellent for outpatient aneurysm and stenosis screening.
- Digital subtraction angiography (DSA): the gold standard for vascular detail and the platform for endovascular treatment.
- Carotid duplex ultrasound: first-line for grading extracranial ICA stenosis.
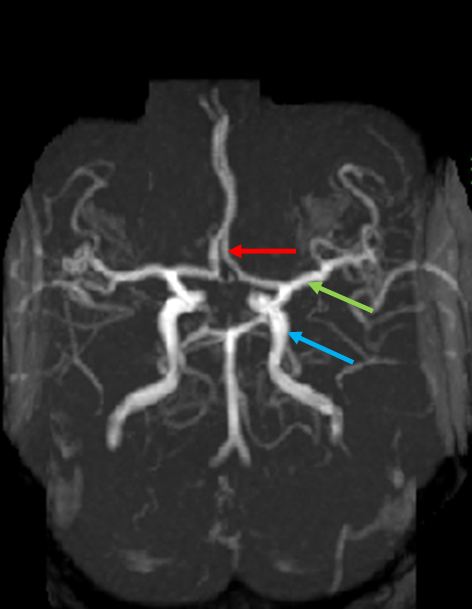
On an inferior (basal) view or MRA, orient yourself by the ring: the two carotids enter anterolaterally and branch into ACA (medial) and MCA (lateral), while the single basilar ascends in the midline to split into the two PCAs posteriorly.
Key Points for Exams – نقاط مهمة للامتحانات
- Two inflow systems feed the brain: internal carotids → anterior circulation (ACA, MCA) and vertebrals → basilar → posterior circulation (PCA + cerebellar arteries), joined by the Circle of Willis.
- Ophthalmic artery (first ICA branch) embolus → amaurosis fugax; carotid duplex is first-line for ICA stenosis.
- ACA infarct → contralateral leg weakness + urinary incontinence; MCA infarct → contralateral face/arm weakness, aphasia (dominant) or neglect (non-dominant), ± hemianopia.
- PCA infarct → contralateral homonymous hemianopia with macular sparing.
- PICA/lateral medulla = Wallenberg syndrome; AICA/lateral pons adds ipsilateral facial palsy and deafness (labyrinthine artery).
- Deep lenticulostriate perforators are end-arteries → lacunar infarcts and the #1 site of hypertensive intracerebral hemorrhage (putamen).
- Watershed (ACA–MCA, MCA–PCA) infarcts follow global hypoperfusion → "man-in-a-barrel" proximal weakness.
- Berry aneurysms arise at bifurcations — ACom is most common; a PCom aneurysm causes a pupil-involving CN III palsy; rupture → subarachnoid hemorrhage.
| Mnemonic – جملة تذكرية | |
|
جملة تذكرية |
| نقاط مهمة للامتحانات – Key Points for Exams | |
ركّز على: الدورة الأمامية (ICA) مقابل الخلفية (vertebrobasilar)، وربط كل شريان بالعجز السريري الموافق له (ACA = الساق، MCA = الوجه/الذراع، PCA = الرؤية). الأم أم التوت (berry aneurysm) في ACom هي الأشيع، وPCom تسبّب شلل العصب الثالث. |
ملاحظة |
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.