Summary
Sideroblastic anemia is a heterogeneous group of disorders characterized by impaired mitochondrial heme synthesis, leading to ineffective erythropoiesis and microcytic, hypochromic (or dimorphic) anemia (MCV < 80 fL). The core mechanism involves the failure to incorporate iron into protoporphyrin IX, causing perinuclear iron accumulation in erythroblasts. Etiologies include hereditary X-linked ALAS2 mutations, acquired clonal myelodysplastic syndromes (MDS-RS), and reversible causes like alcohol toxicity, lead poisoning, isoniazid therapy, and vitamin B6 deficiency. Peripheral blood smear displays basophilic stippling (classic for lead exposure), Pappenheimer bodies, and a dimorphic RBC population.
Diagnosis is confirmed via bone marrow aspirate demonstrating ringed sideroblasts (15% or greater) on Prussian blue stain, accompanied by elevated serum iron, high ferritin, and increased transferrin saturation. Management centers on treating the underlying cause, administering trial pyridoxine (vitamin B6), or chelation (e.g., DMSA for lead, deferasirox for iron overload); iron supplementation is strictly contraindicated.
Overview
Sideroblastic anemia is a heterogeneous group of disorders in which the bone marrow cannot incorporate iron into heme. The result is a triad of: (1) defective heme synthesis inside erythroblasts, (2) mitochondrial iron accumulation encircling the nucleus → ringed sideroblasts, and (3) ineffective erythropoiesis — precursors die in the marrow, so anemia develops despite abundant iron.
- Anemia type: usually microcytic, hypochromic (can be normocytic or dimorphic, especially with alcohol/MDS).
- Paradox: iron utilization fails, but absorption continues → progressive systemic iron overload (hemochromatosis-like picture).
- Hallmark labs: ↑ serum iron, ↑ ferritin, ↑ transferrin saturation, ↓ TIBC — the mirror image of iron deficiency.
- Diagnostic finding: ringed sideroblasts on bone marrow Prussian blue stain.
Pathophysiology
The heme synthesis pathway
Every cause of sideroblastic anemia maps onto one step of heme synthesis:
- Glycine + Succinyl-CoA → δ-ALA by ALA synthase (mitochondria; rate-limiting; needs vitamin B6 as cofactor). Impaired by B6 deficiency, isoniazid, and the X-linked ALAS2 defect.
- δ-ALA → Porphobilinogen by ALA dehydratase (cytoplasm). Inhibited by lead.
- Several cytoplasmic steps → Protoporphyrin IX.
- Back in mitochondria: Protoporphyrin IX + Fe²⁺ → Heme by ferrochelatase. Inhibited by lead.
When any step fails, iron is still shuttled into mitochondria but cannot be loaded onto protoporphyrin → it piles up around the nucleus (the ringed sideroblast). Defective precursors undergo intramedullary death (ineffective erythropoiesis), hepcidin is suppressed, and intestinal iron absorption rises — driving the iron overload.
| Lead blocks two enzymes — "ALA–Fe" | |
→ Heme synthesis fails at both ends → microcytic anemia + basophilic stippling. |
جملة تذكرية |
| ملاحظة أساسية | |
|
المشكلة الجوهرية ليست نقص الحديد، بل فشل إدخال الحديد في حلقة الهيم داخل الميتوكوندريا، فيتراكم الحديد على شكل حلقة حول النواة (Ring sideroblast) مع تكوّن دم غير فعّال (ineffective erythropoiesis)، أي فقر دم رغم وفرة الحديد. |
ملاحظة |
Etiology & Clinical Presentation
Group the causes by the "Rule of 3": hereditary, acquired–reversible (drugs/toxins/nutrition), and acquired–clonal (bone marrow disease). For exams, anchor on the high-yield quartet: Alcohol, Lead, Isoniazid, and MDS — alcohol is the commonest acquired cause overall, while MDS dominates in the elderly.
| Causes of Sideroblastic Anemia — the "Rule of 3": Hereditary · Acquired–Reversible · Acquired–Clonal | |
| Hereditary | Congenital |
| X-linked (ALAS2 mutation) | Most common inherited form; defective δ-aminolevulinic acid synthase (ALAS2). Young males; often pyridoxine-responsive. |
| Mitochondrial syndromes | Rare (e.g., Pearson syndrome). |
| Acquired – Reversible | Drugs / Toxins / Nutrition |
| Alcohol | Most common acquired cause worldwide; mitochondrial toxin + impairs B6 metabolism. |
| Lead | Inhibits ALA dehydratase + ferrochelatase → basophilic stippling. |
| Isoniazid (INH) | Antagonizes vitamin B6 → blocks ALA synthase; prevented by co-prescribing B6. |
| Chloramphenicol / Linezolid | Inhibit mitochondrial protein synthesis. |
| Copper deficiency | Excess zinc intake or bariatric surgery; copper needed for iron transport. |
| Acquired – Clonal | Bone marrow disease |
| Myelodysplastic syndrome (MDS-RS) | Elderly; SF3B1 mutation; ring sideroblasts ≥15%; may progress to AML. |
| Drugs/toxins causing sideroblastic anemia — "CIAL" | |
Plus Linezolid, Copper deficiency, vitamin B6 deficiency. |
جملة تذكرية |
The isoniazid mechanism is a recurring exam target: INH inhibits pyridoxine phosphokinase, blocking conversion of B6 to its active cofactor needed by ALA synthase.

Clinical presentation
- General anemia: fatigue, weakness, pallor, exertional dyspnea, palpitations, dizziness.
- Iron overload (chronic cases — looks like secondary hemochromatosis): bronze skin pigmentation, hepatomegaly/liver dysfunction, diabetes mellitus, hypogonadism, cardiomyopathy and arrhythmias.
Clues to the specific cause
- Lead: abdominal colic, constipation, peripheral neuropathy (wrist/foot drop in adults), encephalopathy and developmental delay in children, gingival lead line (Burton lines); smear shows basophilic stippling.
- Alcohol: coexisting macrocytosis (dimorphic smear) and signs of liver disease.
- Isoniazid: patient on anti-TB therapy without B6 supplementation.
- MDS: elderly patient, frequently with cytopenias/pancytopenia.
- Hereditary (X-linked): young male, family history, possible splenomegaly.
The lead smear finding is highly testable: 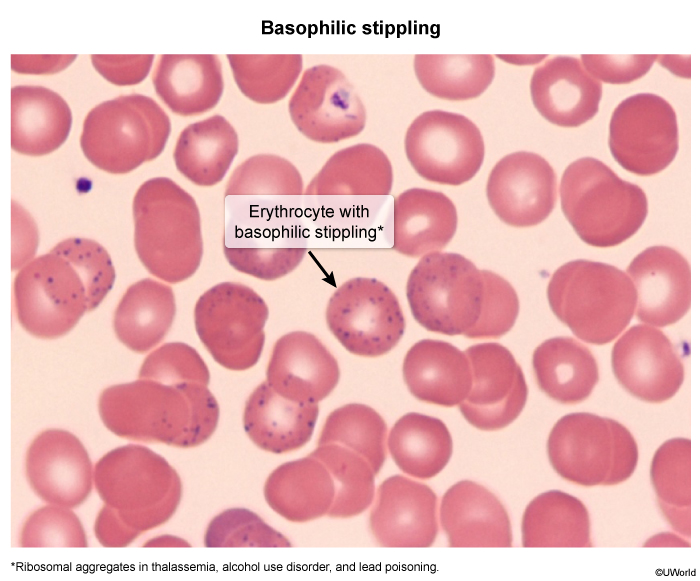
| Important – فكرة سؤال | |
Classic lead vignette: a child in an old house with abdominal pain, constipation, irritability, and learning problems, plus a microcytic anemia. Smear shows basophilic stippling; gums show a lead line (Burton lines). → Diagnosis: lead poisoning (a sideroblastic anemia). Confirm with a blood lead level. Treat with chelation (DMSA orally; EDTA ± dimercaprol if severe/encephalopathy). |
تذكر |
| نقطة امتحانية | |
أكثر سبب مكتسب شيوعاً هو الكحول (Alcohol)، وأكثر سبب وراثي شيوعاً هو طفرة ALAS2 المرتبطة بالكروموسوم X (ذكر صغير السن). تذكّر الرباعية عالية الورود: الكحول، الرصاص، الأيزونيازيد، ومتلازمة خلل التنسج النقوي (MDS). |
ملاحظة |
Diagnostic Approach
Lead with the iron-study signature — it is the single fastest discriminator and the most heavily tested fact:
- Serum iron: ↑ high
- Ferritin: ↑ high
- TIBC / transferrin: ↓ low or normal
- Transferrin saturation: ↑↑ markedly high (often > 50%)
- Reticulocytes: inappropriately low (ineffective erythropoiesis)
| Iron studies — "Sideroblastic = Surplus iron" | |
Exact mirror image of iron deficiency anemia. Microcytic anemias = TICS: Thalassemia, Iron deficiency, Chronic disease, Sideroblastic. |
جملة تذكرية |
| فخ امتحاني | |
|
نمط الحديد في هذا المرض هو عكس فقر الدم بعوز الحديد تماماً (↑ حديد، ↑ فيريتين، ↓ TIBC، ↑↑ تشبّع الترانسفيرين)، مما يجعله سؤالاً متكرراً للتمييز بينهما. |
ملاحظة |
The four microcytic anemias side-by-side
Any microcytic anemia (MCV < 80 fL) is worked through the TICS differential, and iron studies separate them at a glance:
| Microcytic Anemia — Master Differential (iron studies) | ||||
|---|---|---|---|---|
| Feature | Iron deficiency (IDA) | Anemia of chronic disease | Thalassemia | Sideroblastic |
| Serum iron | ↓ Low | ↓ Low | Normal | ↑ High |
| Ferritin | ↓ Low | ↑ High | Normal | ↑ High |
| TIBC | ↑ High | ↓ Low | Normal | ↓ Low / Normal |
| Transferrin saturation | ↓ Low | ↓ Low / normal | Normal / high | ↑↑ High |
| RDW | ↑ High | Normal | Normal | Often ↑ (dimorphic) |
| Key smear/marrow clue | Pencil & target cells | Often normocytic | Target cells; ↑HbA₂ (β-thal minor) | Basophilic stippling (lead); ringed sideroblasts in marrow |
See the iron studies in microcytic anemia comparison for the full ferritin / TIBC / saturation breakdown, and the IDA vs α-thalassemia vs β-thalassemia minor table for the RBC count and electrophoresis features that separate the normal-iron microcytic anemias.
Smear and bone marrow findings
- Peripheral smear: hypochromic, microcytic RBCs, often a dimorphic population; basophilic stippling (lead); Pappenheimer bodies (iron-containing granules).
- Bone marrow (Prussian blue) — diagnostic: ringed sideroblasts ≥ 15%, i.e., ≥ 5 iron granules encircling ≥ one-third of the nuclear circumference.
- If lead suspected: ↑ blood lead level, ↑ zinc protoporphyrin, ↑ urinary δ-ALA.
The marrow hallmark — iron studded around the nucleus on Prussian blue stain: 
On the peripheral smear, the corresponding iron inclusions are 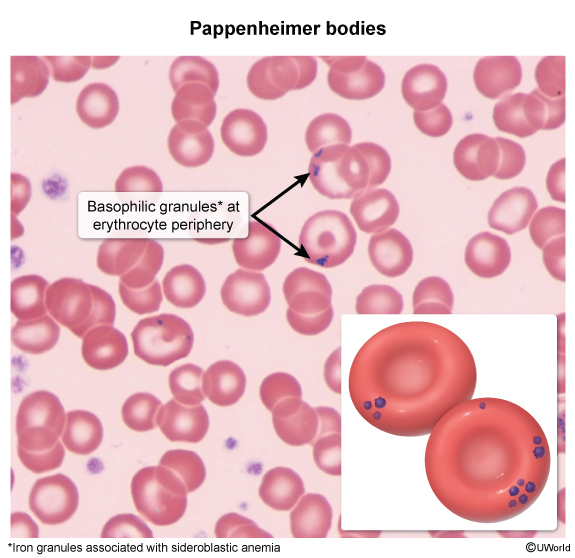
Management & Complications
Management has three pillars: treat the cause, manage iron overload, and supportive care — with complications driven mainly by chronic iron loading.
1. Treat the underlying cause
- Hereditary (X-linked, ALAS2): pyridoxine (vitamin B6) 50–200 mg PO daily, often lifelong; many respond partially.
- Alcohol-induced: stop alcohol → anemia usually reverses over weeks.
- Isoniazid-induced: add/increase pyridoxine 25–50 mg PO daily; always co-prescribe B6 with INH to prevent it.
- Lead poisoning: remove exposure + chelation — DMSA (succimer) PO for moderate levels; CaNa₂-EDTA ± dimercaprol (BAL) for severe disease/encephalopathy.
- Copper deficiency: copper replacement and stop excess zinc.
- MDS-RS: supportive transfusions; luspatercept, erythropoiesis-stimulating agents, or hypomethylating agents (azacitidine); allogeneic stem cell transplant in selected younger patients.
For the marrow features and classification of the clonal form, refer to the clinical features of myelodysplastic syndrome, which covers MDS-RS and its SF3B1 association.
2. Manage iron overload
- Iron chelation when ferritin is markedly elevated or after repeated transfusions: deferasirox 20 mg/kg PO daily, deferiprone, or deferoxamine (SC/IV infusion).
- Never give iron supplements — the defect is iron utilization, not iron lack; supplementation only accelerates overload.
| ملاحظة سريرية هامة | |
|
إعطاء الحديد لهؤلاء المرضى ممنوع تماماً لأنه يفاقم فرط حمل الحديد (iron overload)؛ المشكلة في استخدام الحديد وليست في نقصه. |
ملاحظة |
3. Supportive care
- Transfuse for symptomatic anemia, but sparingly to limit iron loading.
- Folic acid supplementation (high marrow turnover).
- Monitor end-organ damage; treat infections and vaccinate.
| Note – ملاحظة | |
|
Patients on isoniazid (INH) for tuberculosis should routinely receive pyridoxine (vitamin B6) 25–50 mg PO daily to prevent both peripheral neuropathy and sideroblastic anemia. |
ملاحظة |
Complications
- Secondary iron overload (hemosiderosis / hemochromatosis-like): liver — hepatomegaly, cirrhosis, hepatocellular carcinoma; heart — cardiomyopathy, heart failure, arrhythmias; endocrine — diabetes mellitus, hypogonadism, hypothyroidism; skin — bronze pigmentation.
- Transfusion-related: alloimmunization, infection, additional iron load.
- Progression to AML in MDS-associated disease.
- Lead-specific: encephalopathy, peripheral neuropathy, nephropathy, and developmental delay in children.
High-Yield Exam Summary
The must-know facts, distilled for rapid review:
| Key Points for Exams – نقاط مهمة للامتحانات | |
|
تذكر |
| خلاصة سريعة | |
إذا رأيت فقر دم صغير الكريات (microcytic) مع ارتفاع الحديد والفيريتين وتشبّع الترانسفيرين، فكّر فوراً بفقر الدم الحديدي الأرومي (sideroblastic)، وابحث عن السبب: كحول، رصاص، أيزونيازيد، أو MDS — والعلاج يبدأ دائماً بإزالة السبب وإعطاء B6 لا الحديد. |
ملاحظة |
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.