Summary
Lead poisoning (plumbism) is a heavy-metal toxicity that causes a microcytic, hypochromic, sideroblastic anemia (MCV < 80 fL) by disrupting heme synthesis. Lead directly inhibits cytoplasmic ALA dehydratase (elevating urine delta-ALA) and mitochondrial ferrochelatase (elevating zinc protoporphyrin), preventing iron incorporation into heme, while also inhibiting RBC 5'-nucleotidase to cause ribosomal RNA aggregation. Clinical manifestations include neurocognitive decline, encephalopathy, and abdominal colic in children, alongside wrist/foot drop (radial/peroneal motor neuropathy), saturnine gout, and Burton gingival lines in adults. Peripheral blood smear characteristically shows coarse basophilic stippling with normal serum iron and ferritin. Diagnosis is confirmed via a venous blood lead level (BLL). Management requires source abatement; chelation therapy is indicated for moderate toxicity (oral succimer for BLL 45–69 ug/dL) or severe toxicity (IM dimercaprol followed by IV calcium disodium EDTA for BLL 70 ug/dL or greater/encephalopathy).
Overview
Lead poisoning (plumbism) is toxic exposure to lead (Pb) that inhibits several enzymes of the heme synthesis pathway, producing a microcytic, hypochromic, sideroblastic anemia with coarse basophilic stippling on the peripheral smear. It is the most common heavy-metal poisoning in children and a classic occupational toxin in adults.
Top exposure scenarios (risk factors)
- Lead-based paint & dust — children (#1 source): chips/dust in homes built before 1978, amplified by pica and hand-to-mouth behavior; low socioeconomic status and immigrant/international-adoptee status raise risk.
- Occupational exposure — adults: battery manufacturing, ammunition/firing ranges, smelting, soldering, construction/demolition, radiator repair, and pottery/stained-glass glazing.
- Contaminated water & soil: old lead pipes/solder and leaded soil; also imported toys, kohl cosmetics, traditional remedies, and moonshine distilled in lead-soldered stills.
Pathophysiology
Core mechanism — inhibition of heme synthesis
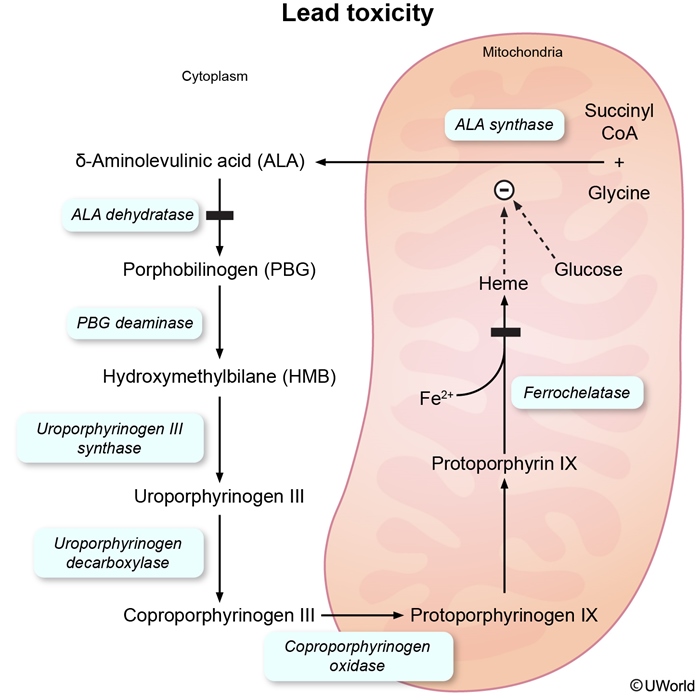
Lead is absorbed via the GI tract (children absorb ~50%) or by inhalation (adults), then distributed to blood (98% bound to RBCs), soft tissue, and bone (half-life ≈ 20–30 years). The hallmark toxicity is two enzyme blocks:
- ↓ ALA dehydratase (cytoplasm) → δ-aminolevulinic acid cannot become porphobilinogen → ↑ urine δ-ALA.
- ↓ Ferrochelatase (mitochondria) → iron cannot be inserted into protoporphyrin IX → mitochondrial iron accumulates around the nucleus (ring sideroblasts) and protoporphyrin binds zinc instead → ↑ zinc protoporphyrin (ZPP).
- Net effect → ↓ heme → microcytic, hypochromic sideroblastic anemia.
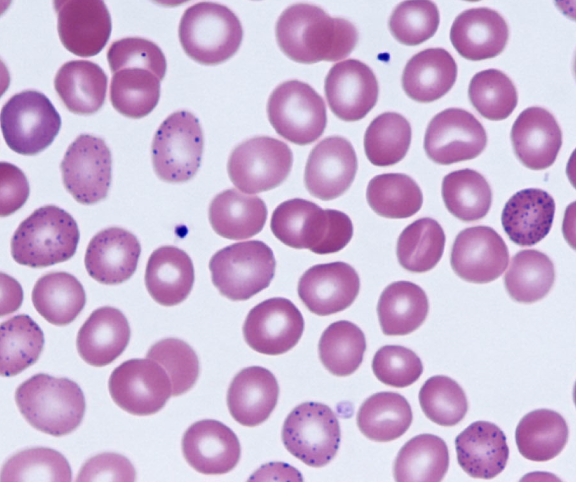
- Inhibition of RBC 5′-nucleotidase → undegraded ribosomal RNA aggregates → coarse basophilic stippling.
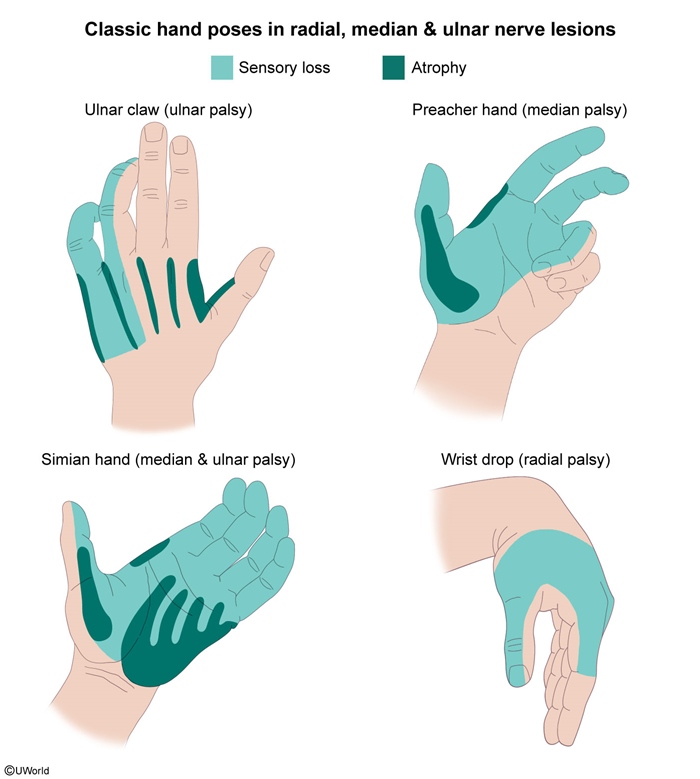
Lead also binds sulfhydryl groups and displaces Ca²⁺, driving peripheral motor demyelination (wrist/foot drop), cerebral edema/encephalopathy, and proximal tubular injury (Fanconi-like syndrome, saturnine gout).
Clinical Presentation & Complications
Lead toxicity is often insidious or asymptomatic, especially with low-level chronic exposure. Manifestations track four organ systems — nervous system, GI tract, blood, kidney — with a different emphasis in children versus adults.
| Clinical Presentation: Children vs Adults | ||
|---|---|---|
| System | Children (neurocognitive predominant) | Adults (occupational predominant) |
| Neurologic | ↓ IQ, irritability, behavioral problems, developmental regression; severe → encephalopathy, seizures, coma | Motor peripheral neuropathy → wrist drop, foot drop; headache, fatigue, memory loss |
| Gastrointestinal | Abdominal pain, anorexia, constipation, vomiting | Lead colic — crampy abdominal pain, constipation, metallic taste |
| Hematologic | Microcytic anemia + coarse basophilic stippling | Microcytic anemia + coarse basophilic stippling |
| Renal / Metabolic | Less common (seen with chronic exposure) | Chronic interstitial nephritis, saturnine gout, hypertension |
| Classic signs | Burton lines on gingiva; dense metaphyseal bands on long-bone X-ray | Burton lines on gums; infertility, ↓ libido, miscarriage |
High-yield buzzwords to lock in: wrist drop and foot drop (adult motor neuropathy, radial and peroneal nerves first), Burton lines (blue-grey gingival lead lines), and lead colic (crampy, recurrent abdominal pain).
Serious complications, by system
- Neurologic (most concerning in children): permanent ↓ IQ, learning disability, ADHD-like behavior; lead encephalopathy (BLL > 70–100 µg/dL) → cerebral edema, seizures, coma, death. Adults → persistent motor neuropathy (wrist/foot drop).
- Renal: proximal tubular dysfunction → Fanconi-like syndrome (aminoaciduria, glycosuria, phosphaturia); chronic interstitial nephritis, ↓ GFR, hypertension; impaired vitamin-D 1-α-hydroxylation; saturnine gout (↓ urate excretion).
- Hematologic: chronic microcytic, hypochromic, sideroblastic anemia.
- Reproductive: infertility, ↓ sperm count, miscarriage, prematurity; lead crosses the placenta → fetal neurotoxicity.
Diagnostic Approach
Step 1 — Confirm with a blood lead level (BLL)
- First-line & gold standard: venous blood lead level (a capillary screen that is elevated must be confirmed venously).
- No safe level exists in children; the CDC blood lead reference value = ≥ 3.5 µg/dL (elevated).
- Targeted screening at 12 and 24 months in high-risk children (Medicaid, pre-1978 housing, immigrant/adoptee, affected sibling/playmate).
Step 2 — Supportive labs & imaging
- CBC / smear: microcytic, hypochromic anemia with coarse basophilic stippling.
- Iron studies: normal serum iron, ferritin, and TIBC — the pivotal distinction from iron deficiency.
- Zinc protoporphyrin (ZPP): ↑.
- Urine δ-aminolevulinic acid (ALA): ↑.
- Bone marrow (rarely needed): ring sideroblasts on Prussian blue.
- Imaging: abdominal X-ray → radiopaque paint chips in the colon (symptomatic children); long-bone X-ray → dense metaphyseal "lead lines" (represents calcium, not lead).
| ملاحظة سريرية – Clinical Note | |
|
في التسمم بالرصاص، يكون فقر الدم صغير الكريات لكن مخزون الحديد (الفيريتين) طبيعياً، وهذه هي النقطة المفصلية للتفريق بينه وبين فقر الدم بعوز الحديد. |
ملاحظة |
Differential diagnosis — the microcytic anemias (TAILS)
Lead poisoning is one of the "TAILS" microcytic anemias: Thalassemia, Anemia of chronic disease, Iron deficiency, Lead poisoning, Sideroblastic anemia. The single master table below separates them by iron studies and smear:
| Differential Diagnosis of Microcytic Anemia (TAILS) | ||||
|---|---|---|---|---|
| Feature | Lead poisoning | Iron deficiency | Thalassemia | Sideroblastic |
| Serum iron | Normal | ↓ | Normal | ↑ |
| Ferritin | Normal | ↓ | Normal / ↑ | ↑ |
| TIBC | Normal | ↑ | Normal | ↓ |
| RDW | Normal / ↑ | ↑ | Normal | ↑ |
| Basophilic stippling | Yes (coarse) | No | Yes (mild) | Yes |
| Distinguishing clue | Exposure Hx, ↑ ZPP, ↑ urine ALA | Pica, koilonychia, low ferritin | Family Hx, target cells, Hb electrophoresis | Ring sideroblasts on marrow |
Other look-alikes
- Acute intermittent porphyria: abdominal pain + neuro symptoms + ↑ ALA, but ↑ porphobilinogen, NO anemia, and NO basophilic stippling.
- Howell–Jolly bodies (asplenia): a single, large nuclear remnant — versus the multiple scattered blue dots of basophilic stippling.
Management
Step 1 — Remove the source (most important)
- Environmental investigation + lead abatement (home inspection, occupational source control).
- Public-health notification — lead poisoning is a reportable disease.
- Nutritional counseling: replete iron, calcium, vitamin C, and zinc (deficiencies increase lead absorption).
Step 2 — Chelation, stratified by BLL
| Management of Lead Poisoning by Blood Lead Level (BLL): Source removal + public-health reporting are mandatory at EVERY level | |
| Mild | BLL < 45 µg/dL |
| No chelation | Environmental investigation + lead abatement, nutritional counseling (iron, calcium, vitamin C, zinc), serial BLL monitoring |
| Moderate | BLL 45–69 µg/dL |
| Oral chelation | Succimer (DMSA) PO × 19 days; D-penicillamine is an alternative |
| Severe | BLL ≥ 70 µg/dL or any encephalopathy |
| Dual parenteral chelation | Dimercaprol (BAL) IM + calcium disodium EDTA IV; hospitalize, ICU for encephalopathy |
See the Treatment of Asymptomatic Lead Toxicity by Blood Lead Level for the exact chelator and threshold at each band.
Key chelation pearls
- Dimercaprol (BAL) must be given BEFORE EDTA in encephalopathy — EDTA alone mobilizes lead from bone and can worsen CNS toxicity.
- Dimercaprol is contraindicated in peanut allergy (peanut-oil vehicle) and G6PD deficiency.
- Adults: chelate when BLL ≥ 80 µg/dL (asymptomatic) or ≥ 50 µg/dL with symptoms.
- Avoid oral iron co-administration with succimer (forms a toxic complex).
| فخ امتحاني – Exam Trap | |
|
يجب إعطاء الدايمركابرول (BAL) قبل الـ EDTA في حالات الاعتلال الدماغي لمنع تفاقم السمية العصبية. |
ملاحظة |
High-Yield Exam Pearls
The highest-yield, board-tested facts about plumbism, consolidated for rapid review.
- Buzzword smear: coarse basophilic stippling + microcytic anemia with normal iron studies (ferritin normal).
- First diagnostic step: venous blood lead level (gold standard).
- Encephalopathy rule: give BAL before EDTA.
- Child clue: pre-1978 housing + pica → ↓ IQ + abdominal pain. Adult clue: occupational exposure → wrist/foot drop, lead colic, HTN.
| Mnemonic — Clinical picture of lead poisoning ("LEAD") | |
Lead lines on gingiva (Burton) and on bone metaphyses Treatment recall: Succimer for the Suckers (kids, moderate); BAL + EDTA for the BADly poisoned (severe/encephalopathy). |
جملة تذكرية |
| Mnemonic — Enzymes blocked by Lead ("ALA Ferry") | |
|
جملة تذكرية |
| Important — Question Idea: Lead vs Iron Deficiency | |
A child from an old house (pre-1978) presents with abdominal pain, irritability, and microcytic anemia → think lead poisoning, not iron deficiency.
|
تذكر |
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.