Summary
Lymphomas are malignant, clonal proliferations of lymphocytes arising in lymphoid tissues, divided into Hodgkin lymphoma (HL) and Non-Hodgkin lymphoma (NHL). HL classically presents in young adults with painless, contiguous cervical lymphadenopathy, B symptoms (fever, night sweats, weight loss), and Reed-Sternberg cells (CD15+, CD30+ "owl-eye" appearance). NHL comprises diverse B-cell (~85%) or T-cell malignancies featuring non-contiguous spread and extranodal disease (e.g., gastric MALT linked to H. pylori, or translocations like t(14;18) BCL-2 in follicular and t(8;14) c-MYC in Burkitt). An excisional lymph node biopsy is the gold standard diagnostic test (fine-needle aspiration is inadequate). Standard management relies on ABVD for HL and R-CHOP for aggressive B-cell NHL (DLBCL), while early gastric MALT requires H. pylori eradication. Long-term survivors face high risks for secondary malignancies and cardiovascular complications.
Overview & Key Differences
Lymphomas are malignant, clonal tumors of lymphocytes arising primarily in lymph nodes, spleen, and extranodal lymphoid tissue. They divide into two families that look similar at the bedside (painless lymphadenopathy + B symptoms) but differ fundamentally in pathology, pattern of spread, and prognosis:
- Hodgkin lymphoma (HL): defined by the Reed–Sternberg (RS) cell (CD15+, CD30+). Young adults, painless cervical/supraclavicular nodes, contiguous spread, almost always nodal, and highly curable.
- Non-Hodgkin lymphoma (NHL): a heterogeneous group of B-cell (~85%) or T-cell malignancies without RS cells. Older adults, non-contiguous spread, frequent extranodal disease, ~5× more common than HL, and ranging from indolent to highly aggressive.
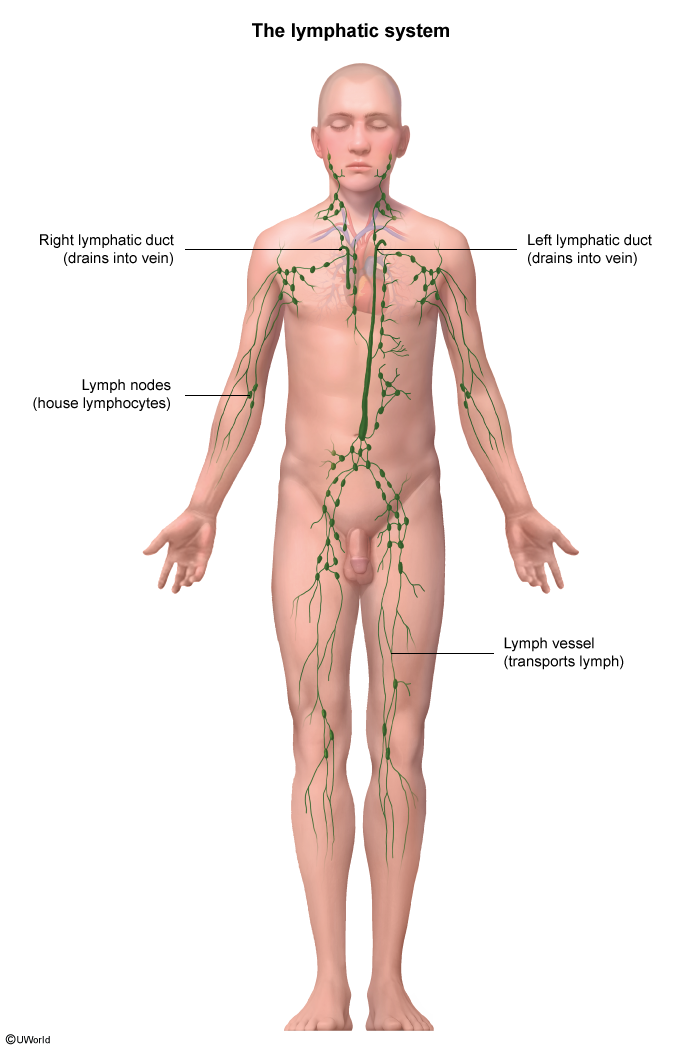
The lymphatic network below explains why disease classically tracks along nodal chains and why HL — but rarely NHL — spreads in an orderly, contiguous fashion.
Master comparison
| Hodgkin vs Non-Hodgkin Lymphoma — Master Comparison | ||
|---|---|---|
| Feature | Hodgkin Lymphoma (HL) | Non-Hodgkin Lymphoma (NHL) |
| Age | Bimodal: 15–35 y and >55 y | Median >60 y; rises steadily with age |
| Key cell | Reed–Sternberg cell (CD15+, CD30+) | Clonal B-cell (~85%) or T-cell; no RS cells |
| Spread | Contiguous & orderly (node → adjacent node) | Non-contiguous; 'skip' lesions |
| Extranodal involvement | Rare — almost always nodal | Common (GI tract, skin, CNS, marrow) |
| Stage at diagnosis | Usually localized (limited stage) | Often disseminated (advanced) at presentation |
| B symptoms | Common; prognostically important | Variable; more frequent with aggressive subtypes |
| First-line therapy | ABVD ± involved-field radiation | R-CHOP (aggressive B-cell); watch-and-wait (indolent) |
| Prognosis | Highly curable (~85–95% in early stage) | Subtype-dependent: indolent (incurable, long survival) vs aggressive (curable) |
Risk factors
Hodgkin lymphoma:
- EBV infection — history of infectious mononucleosis (strongest with mixed-cellularity subtype).
- HIV / immunosuppression.
- Family history (affected sibling).
Non-Hodgkin lymphoma — the "Rule of 3" high-yield associations:
- Immunosuppression: HIV/AIDS (DLBCL, primary CNS lymphoma, Burkitt), post-transplant (PTLD), congenital immunodeficiency.
- Chronic infection (viral/bacterial): EBV → Burkitt and primary CNS lymphoma; H. pylori → gastric MALT lymphoma; (also HTLV-1 → adult T-cell, HCV → marginal zone).
- Autoimmune disease: Sjögren syndrome (MALT), Hashimoto thyroiditis, SLE, RA.
The Sjögren link is a recurrent exam item: chronic lymphocytic stimulation drives B-cell marginal zone (MALT) lymphoma. See the Sjögren syndrome extraglandular manifestations for the autoimmune features that flag this risk, and the Hodgkin lymphoma epidemiology and manifestations overview for the bimodal age pattern and EBV association.
Clinical Presentation & Subtypes
Shared presentation
- Painless lymphadenopathy — firm, rubbery, non-tender nodes. HL favors cervical/supraclavicular chains; NHL involves any region, often multiple/diffuse sites.
- B symptoms — fever >38°C, drenching night sweats, unintentional weight loss >10% over 6 months.
- Hepatosplenomegaly, fatigue, pruritus.
| Important – فكرة سؤال | |
|
B symptoms = the triad of fever >38°C, drenching night sweats, and unintentional weight loss >10% of body weight over 6 months. Pruritus and fatigue are not B symptoms and do not add the 'B' suffix to the Ann Arbor stage. فخ امتحاني: الحكة (pruritus) والتعب ليست من الأعراض B ولا تُضاف للمرحلة، حتى لو كانت شائعة في لمفوما هودجكين. |
تذكر |
HL-specific clues
- Pel–Ebstein fever — cyclical fever every 1–2 weeks.
- Alcohol-induced nodal pain (classic, rare).
- Mediastinal mass (esp. nodular sclerosing in young women) → may cause SVC syndrome.
NHL-specific clues
- Extranodal disease is common: GI tract (most common extranodal site), skin (mycosis fungoides/Sézary), CNS (primary CNS lymphoma in HIV), Waldeyer's ring, testis, thyroid.
- Bone marrow involvement → cytopenias.
- Burkitt lymphoma: rapidly enlarging jaw mass (endemic African) or abdominal mass (sporadic).
Hodgkin lymphoma subtypes
All classical HL subtypes share the Reed–Sternberg cell — a large, binucleated lymphocyte with eosinophilic nucleoli giving the "owl-eye" look (CD15+, CD30+, CD20−, CD45−) sitting in a reactive background.

- Nodular sclerosing — most common (~70%); young women, mediastinal mass, "lacunar cells"; excellent prognosis.
- Mixed cellularity — older adults, HIV/EBV+; many RS cells; intermediate prognosis.
- Lymphocyte-rich — few RS cells → best prognosis.
- Lymphocyte-depleted — many RS cells → worst prognosis; elderly, HIV+.
- Nodular lymphocyte-predominant (non-classical) — "popcorn cells," CD20+, CD15−, CD30−; behaves like indolent B-cell NHL; excellent prognosis.
| Mnemonic – جملة تذكرية — Reed–Sternberg markers | |
|
"15 and 30 owl-eye twins" → RS cells are CD15+ and CD30+, binucleated ('owl eyes'), and CD20− / CD45−. |
جملة تذكرية |
Non-Hodgkin lymphoma subtypes (highest-yield)
B-cell NHL (~85%):
- Diffuse large B-cell lymphoma (DLBCL) — most common NHL; aggressive but curable; rapidly enlarging mass in older adults; treat with R-CHOP.
- Follicular lymphoma — most common indolent NHL; t(14;18) → BCL-2 overexpression (anti-apoptosis); waxing/waning nodes; may transform to DLBCL.
- Burkitt lymphoma — highly aggressive; t(8;14) → c-MYC; "starry sky" histology; Ki-67 ≈ 100%; endemic (jaw/EBV), sporadic (abdominal), HIV-related.
- Mantle cell lymphoma — aggressive, older men; t(11;14) → cyclin D1; CD5+ (like CLL but CD23−).
- Marginal zone / MALT lymphoma — indolent; chronically inflamed tissue (gastric/H. pylori, salivary/Sjögren, thyroid/Hashimoto); t(11;18).
- Primary CNS lymphoma — DLBCL of the brain in HIV/AIDS; EBV-driven; solitary ring-enhancing lesion.
T-cell NHL (~15%):
- Adult T-cell leukemia/lymphoma (ATLL) — HTLV-1; skin lesions, hypercalcemia, lytic bone lesions.
- Mycosis fungoides / Sézary syndrome — cutaneous T-cell lymphoma; skin patches/plaques; "cerebriform" Sézary cells in blood.
Two classic histologies anchor the B-cell subtypes — the orderly neoplastic follicles of follicular lymphoma and the "starry sky" Burkitt lymphoma. For the HIV-associated brain mass, the primary CNS lymphoma vs toxoplasmosis differential separates the two leading ring-enhancing lesions in AIDS.
Defining translocations
Most NHL translocations juxtapose a partner oncogene with the immunoglobulin heavy-chain locus on chromosome 14, driving constitutive expression.
| Key NHL Translocations — High-Yield | ||
|---|---|---|
| Subtype | Translocation | Gene / Protein |
| Follicular lymphoma | t(14;18) | BCL-2 (anti-apoptosis) |
| Burkitt lymphoma | t(8;14) | c-MYC |
| Mantle cell lymphoma | t(11;14) | Cyclin D1 |
| MALT lymphoma | t(11;18) | API2–MALT1 |
| DLBCL | Variable | BCL-6, BCL-2, MYC |
| Mnemonic – جملة تذكرية — NHL translocations | |
|
"8–14 Bursts c-MYC, 11–14 Mantles Cyclin, 14–18 Follicles Block apoptosis"
|
جملة تذكرية |
Diagnostic Workup & Staging
Step 1 — Initial workup
- Serum: CBC (cytopenias if marrow involved; eosinophilia in HL); LDH — elevated, marker of tumor burden/prognosis (esp. NHL); ESR — prognostic in HL; uric acid, calcium, electrolytes, renal function — baseline tumor-lysis risk.
- Serologies: HIV, HBV, HCV, EBV (risk stratification + safe chemotherapy).
- Peripheral smear: may show circulating abnormal lymphocytes.
Step 2 — Definitive diagnosis: biopsy
- Excisional lymph node biopsy = gold standard — preserves architecture for RS-cell identification and NHL immunophenotyping.
- HL: Reed–Sternberg cells (CD15+, CD30+) in a reactive background of lymphocytes, eosinophils, plasma cells.
- NHL: monoclonal lymphocyte proliferation; classify by immunophenotype (CD20+ → B-cell) and cytogenetics.
| Important – فكرة سؤال | |
Excisional lymph node biopsy is mandatory — it preserves nodal architecture, which is required to identify Reed–Sternberg cells and to subclassify NHL. Fine-needle aspiration (FNA) is inadequate for an initial lymphoma diagnosis because it destroys architecture and yields only a cell suspension. فخ امتحاني: إذا ذُكرت FNA في السؤال كخطوة أولى لتشخيص اللمفوما فهي الإجابة الخاطئة؛ الصحيح هو الخزعة الاستئصالية (excisional biopsy). |
تذكر |
Step 3 — Staging workup
- Imaging: PET/CT of neck/chest/abdomen/pelvis — standard for staging and treatment-response assessment.
- Bone marrow biopsy — for advanced HL and most NHL.
- Lumbar puncture — if CNS risk (Burkitt, lymphoblastic, primary CNS, HIV).
- Pre-treatment organ tests: echocardiogram/MUGA before doxorubicin (cardiotoxicity); PFTs before bleomycin (pulmonary fibrosis).
A bulky mediastinal mass on chest radiograph is a hallmark presentation, especially nodular-sclerosing HL in young adults, and can precipitate SVC syndrome.

Ann Arbor staging
Both HL and NHL use the Ann Arbor system (Cotswolds/Lugano modifications). Stage drives treatment intensity; the "B" suffix worsens prognosis within any stage.
| Ann Arbor Staging (HL and NHL): Modifiers: A = no B symptoms | B = fever, night sweats, >10% weight loss | E = localized extranodal extension | S = splenic involvement | |
| Limited stage | Often curable with combined-modality therapy |
| Stage I | Single lymph node region or single extralymphatic site |
| Stage II | ≥2 node regions on the SAME side of the diaphragm |
| Advanced stage | Chemotherapy-based regimens |
| Stage III | Node regions on BOTH sides of the diaphragm ± spleen |
| Stage IV | Diffuse extranodal involvement (liver, bone marrow, lung) |
- Stage IIA = two cervical + one supraclavicular node, no B symptoms.
- Stage IIIB = nodes above and below the diaphragm + fever and weight loss.
- Stage IVB = bone-marrow involvement + B symptoms (advanced).
Management Principles
Hodgkin lymphoma
- Early stage (I–II): short-course ABVD + involved-field radiation therapy.
- Advanced stage (III–IV): full 6 cycles of ABVD (± radiation to bulky disease).
- Relapsed/refractory: salvage chemotherapy + autologous stem-cell transplant; brentuximab vedotin (anti-CD30) and PD-1 inhibitors (nivolumab, pembrolizumab).
| Mnemonic – جملة تذكرية — ABVD (Hodgkin chemo) | |
|
"A Big Van Drove" → ABVD
|
جملة تذكرية |
Non-Hodgkin lymphoma
- DLBCL / aggressive B-cell NHL: R-CHOP × 6 cycles → cure in ~60–70%. Adding rituximab (anti-CD20 monoclonal antibody) to CHOP is standard of care for any CD20-positive B-cell NHL.
- Burkitt lymphoma: intensive multi-agent chemotherapy + intrathecal CNS prophylaxis + aggressive tumor-lysis prophylaxis (IV hydration, allopurinol or rasburicase).
- Follicular lymphoma (indolent): asymptomatic/low-burden → "watch and wait"; symptomatic → rituximab ± bendamustine or R-CHOP.
- Gastric MALT lymphoma: H. pylori eradication first; radiation/rituximab if no regression.
- CLL/SLL: watch-and-wait if asymptomatic; treat with BTK inhibitors (ibrutinib) or BCL-2 inhibitors (venetoclax) when indicated.
| Mnemonic – جملة تذكرية — R-CHOP (DLBCL chemo) | |
|
Rituximab · Cyclophosphamide · Hydroxydaunorubicin (doxorubicin) · Oncovin (vincristine) · Prednisone. "Rituximab Chops B-cells" → anti-CD20 monoclonal antibody. |
جملة تذكرية |
| Important – فكرة سؤال | |
|
Gastric MALT lymphoma is treated first with H. pylori eradication (triple therapy) — not chemotherapy. Eradication alone induces lymphoma regression in >75% of early, t(11;18)-negative cases. Radiation or rituximab is reserved for non-responders. ملاحظة سريرية: لمفوما MALT المعدية تتراجع باستئصال جرثومة المعدة وحده قبل اللجوء للعلاج الكيماوي. |
تذكر |
When NHL presents as a blood-predominant lymphoproliferation, the differential overlaps with leukemia — review the CLL diagnosis and treatment indications for the flow-cytometry CD5/CD19/CD20/CD23 signature and the symptom-based threshold for starting therapy.
Complications & Prognosis
Disease-related complications
- Bone marrow failure → cytopenias, infections.
- SVC syndrome from a large mediastinal mass (HL, lymphoblastic NHL).
- Spinal cord compression from an epidural mass.
- Tumor lysis syndrome — especially Burkitt and lymphoblastic; may occur spontaneously before chemotherapy.
- Paraneoplastic: hypercalcemia (ATLL), autoimmune hemolytic anemia (CLL/SLL); hyperviscosity (lymphoplasmacytic/Waldenström).
Treatment-related (long-term)
- Second malignancies — AML/MDS (alkylators); after mantle radiation for HL: breast, lung, thyroid cancer.
- Cardiotoxicity (doxorubicin, mediastinal radiation).
- Pulmonary fibrosis (bleomycin).
- Infertility and hypothyroidism (alkylators; neck radiation).
| Important – فكرة سؤال | |
|
In a cured Hodgkin lymphoma survivor, the leading cause of death >10 years after treatment is a second malignancy (breast, lung, thyroid after mantle radiation; AML/MDS after alkylators) or cardiovascular disease — not the lymphoma itself. ملاحظة سريرية: السبب الرئيسي للوفاة بعد أكثر من 10 سنوات هو سرطان ثانوي أو مرض قلبي وعائي وليس اللمفوما. |
تذكر |
Because cure is common, lifelong survivorship surveillance for these late effects is essential — the long-term complications and screening strategies in lymphoma survivors lays out the second-malignancy, cardiac, and endocrine monitoring schedule.
Prognosis
- HL: excellent — 5-yr survival ~85–95% (early stage); ~70–80% (advanced).
- DLBCL: ~60–70% cured with R-CHOP; risk-stratify with the IPI score (age, LDH, performance status, stage, extranodal sites).
- Follicular: indolent but incurable — median survival >15 years.
- Burkitt: highly aggressive yet very chemo-sensitive → curable with intensive therapy.
| Key Points for Exams – نقاط مهمة للامتحانات | |
|
ملاحظة |
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.