Summary
Plasma cell disorders stem from the clonal proliferation of plasma cells secreting monoclonal immunoglobulins (M-protein). Multiple myeloma (MM) is classified by >= 10% clonal bone marrow plasma cells (or plasmacytoma) alongside end-organ damage defined by CRAB features (hyperCalcemia, Renal failure, normocytic Anemia, and lytic Bone lesions). Laboratory and smear hallmarks include rouleaux formation, markedly elevated ESR, an M-spike on serum protein electrophoresis (SPEP), and urine Bence Jones proteins detected via UPEP (not routine dipstick). Bone marrow biopsy is the gold-standard diagnostic test, while bone scans are characteristically negative (lytic, non-osteoblastic disease). Management involves VRd induction (bortezomib, lenalidomide, dexamethasone), autologous stem cell transplantation, and bisphosphonates; urgent plasmapheresis is indicated for hyperviscosity syndrome in Waldenström macroglobulinemia.
Overview
Plasma cell disorders (dyscrasias) are driven by clonal proliferation of plasma cells — the terminal, antibody-secreting form of a B-lymphocyte — that secrete a single monoclonal immunoglobulin or light chain, the M-protein (paraprotein / M-spike). They form a biological spectrum from benign to malignant to deposition disease.
The spectrum (with thresholds)
- MGUS (Monoclonal Gammopathy of Undetermined Significance) — M-protein <3 g/dL, marrow clonal plasma cells <10%, no CRAB. Benign/premalignant; ~1%/year progression to MM.
- Smoldering MM — M-protein ≥3 g/dL OR marrow plasma cells 10–60%, no CRAB. Asymptomatic; ~10%/year progression.
- Multiple myeloma (MM) — malignant clonal plasma cells + CRAB end-organ damage. Highest-yield entity.
- Solitary plasmacytoma — single bone or extramedullary plasma-cell tumor without systemic disease.
- Waldenström macroglobulinemia (WM) — IgM-secreting lymphoplasmacytic lymphoma → hyperviscosity.
- AL amyloidosis — misfolded light chains deposit as amyloid in heart, kidney, nerves, and tongue.
One-liner to recognise MM: an older patient with bone pain, anemia, renal failure, and hypercalcemia.
Epidemiology (high-yield)
- Age: almost always >40; median MM diagnosis ≈ 65–70 years.
- Sex / race: male > female; African ancestry → ~2× MM incidence.
- MGUS is common — present in ~3% of people >50; most never progress.
- MM is the 2nd most common hematologic malignancy (after non-Hodgkin lymphoma) and the most common primary malignancy of bone.
- Risk factors: older age, radiation, obesity, family history, chronic immune stimulation.
Pathophysiology
Pathophysiology
A single malignant plasma-cell clone expands in the bone marrow; damage arises from two mechanisms:
1. Direct marrow infiltration — clonal cells crowd out hematopoiesis → normocytic anemia (± leukopenia, thrombocytopenia); they secrete RANK-L, IL-6, and MIP-1α that activate osteoclasts and suppress osteoblasts → lytic bone lesions, bone pain, hypercalcemia, pathologic fractures.
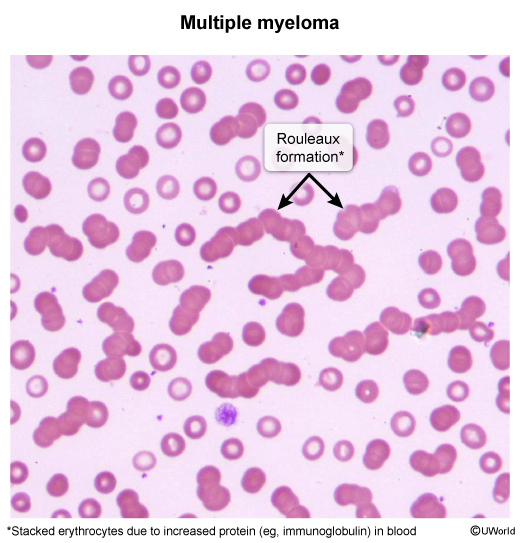
2. Effects of the M-protein — free light chains (Bence Jones protein) precipitate with Tamm–Horsfall protein in renal tubules → cast nephropathy (myeloma kidney); light chains may misfold into AL amyloid; large amounts of intact Ig (especially IgM in WM) → hyperviscosity; the clonal Ig is functionally useless → functional hypogammaglobulinemia → infections with encapsulated bacteria; M-protein coats RBCs → rouleaux and a markedly ↑ ESR.
Virtually all MM is preceded by years of asymptomatic MGUS.
| Mnemonic — Multiple Myeloma (CRAB) | |
|
The four end-organ damage features that define symptomatic multiple myeloma:
Other quick aids: Waldenström = Whopping IgM (hyperviscosity, the only one with retinal “sausage” veins); AL amyloid = Light chains (L for Light, L for AL). |
جملة تذكرية |
Clinical Presentation
Recognising plasma cell disorders means contrasting three distinct presentations: multiple myeloma (CRAB), Waldenström macroglobulinemia (hyperviscosity), and AL amyloidosis (organ deposition).
Multiple myeloma — the CRAB patient
- Bone pain — most common symptom (~70%); back, ribs, hips, worse with movement; may present as a pathologic fracture or vertebral compression.
- Anemia — fatigue, pallor, exertional dyspnea.
- Hypercalcemia — “stones, bones, groans, psychiatric overtones”: polyuria, constipation, confusion, nausea.
- Renal failure — foamy urine, edema, rising creatinine.
- Recurrent infections — sinopulmonary / urinary with encapsulated organisms (S. pneumoniae, H. influenzae) from functional hypogammaglobulinemia.
- Neurologic — spinal cord compression (oncologic emergency), radiculopathy, peripheral neuropathy.
Waldenström macroglobulinemia — the hyperviscosity patient
- No lytic bone lesions and no hypercalcemia — the key contrast with MM.
- Hyperviscosity syndrome — headache, blurred vision, dizziness, mucosal bleeding (epistaxis, gum bleeding), “sausage-link” retinal veins.
- Lymphadenopathy + hepatosplenomegaly — because WM is a lymphoplasmacytic lymphoma.
- May cause IgM-related peripheral neuropathy and type I cryoglobulinemia.
(فخ امتحاني: على عكس المايلوما، الوالدنشتروم لا يسبب آفات عظمية حالة ولا فرط كالسيوم؛ العلامة المميزة هي متلازمة فرط اللزوجة الناتجة عن IgM).
Refer to the hyperviscosity syndrome evaluation and management for the urgent plasmapheresis pathway.
AL amyloidosis — the organ-deposition patient
- Nephrotic syndrome, restrictive cardiomyopathy, hepatomegaly.
- Macroglossia and periorbital purpura — highly characteristic.
- Peripheral / autonomic neuropathy (orthostatic hypotension, carpal tunnel).
Diagnostic Approach
Workup is stepwise: confirm a monoclonal protein, quantify marrow plasma cells, and image the skeleton.
1. Initial labs
- CBC — normocytic, normochromic anemia.
- Peripheral smear — rouleaux formation (RBCs stacked like coins).
- ↑ ESR (often very high), ↑ total protein with a narrow albumin–globulin gap (normal albumin, high globulin).
- ↑ Calcium, ↑ creatinine; normal alkaline phosphatase (lytic, not blastic).
2. Detect & characterise the M-protein
- Serum protein electrophoresis (SPEP) — tall, narrow M-spike in the γ-region (first-line screen).
- Urine protein electrophoresis (UPEP) — Bence Jones free light chains.
- Serum immunofixation — identifies the heavy chain (IgG > IgA) and light chain (κ or λ).
- Serum free light chain (FLC) assay — abnormal κ/λ ratio (most sensitive).
(فخ امتحاني: شريط البول الروتيني لا يكشف بروتينات بنس جونز لأنه يقيس الألبومين فقط. يجب طلب فحص البروتين في البول UPEP).
3. Bone marrow biopsy (clonal-burden confirmation)
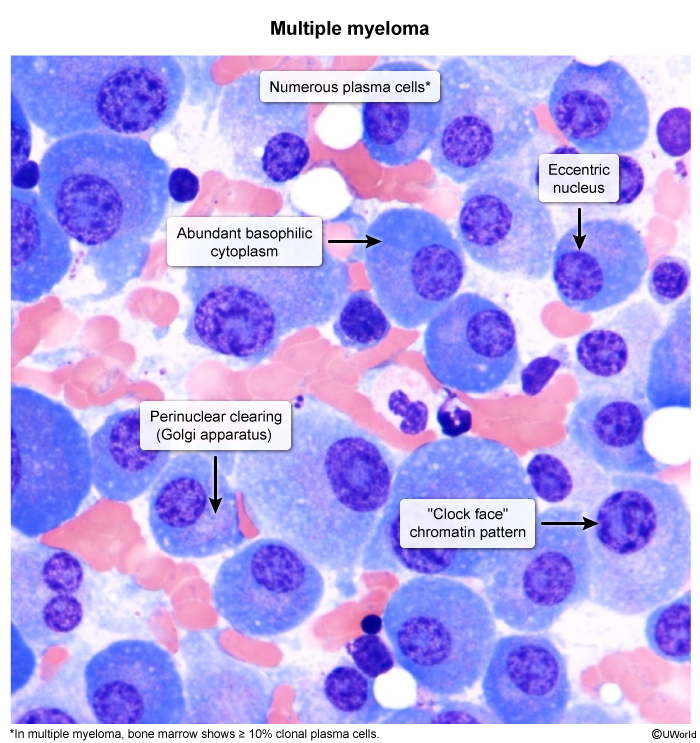
- ≥10% clonal plasma cells meets the diagnostic threshold.
- Morphology: eccentric “clock-face” nucleus, basophilic cytoplasm, perinuclear hof (pale Golgi zone).
4. Imaging
- Preferred: whole-body low-dose CT, MRI, or PET-CT (more sensitive than plain films).
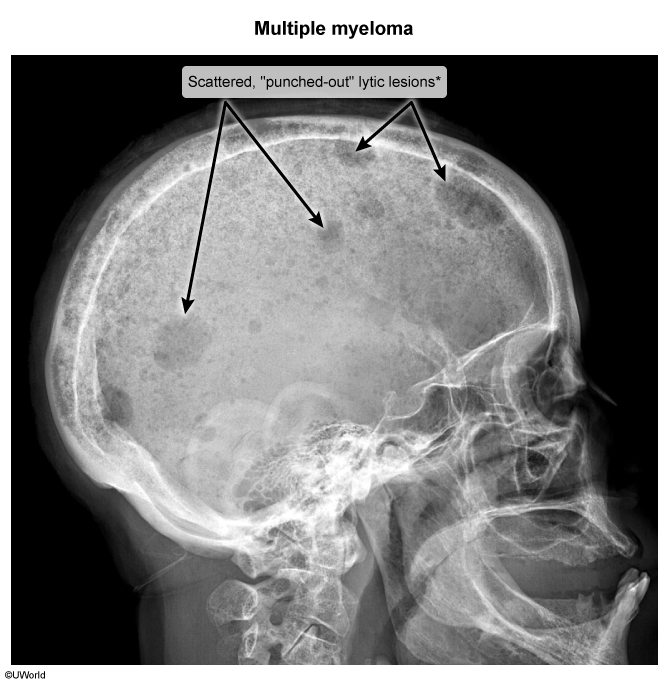
- Classic finding: “punched-out” lytic lesions — skull, spine, ribs, pelvis, long bones.
- Bone scan is typically NEGATIVE and alkaline phosphatase is normal (no osteoblastic reaction).
(ملاحظة سريرية: فحص العظام بالنظائر المشعة يكون سلبياً في المايلوما لأن الآفات حالة للعظم (osteolytic) وليست بانية (osteoblastic)، على عكس معظم النقائل العظمية).
5. Diagnostic criteria (IMWG)
MM requires both: (1) ≥10% clonal plasma cells (or biopsy-proven plasmacytoma) AND (2) one of — CRAB features OR a myeloma-defining event (marrow plasma cells ≥60%, serum FLC ratio ≥100, or >1 focal MRI lesion). See the Diagnostic Criteria for Multiple Myeloma (CRAB) for the full thresholds and myeloma-defining events.
| Master Comparison: MGUS vs Multiple Myeloma vs Waldenström Macroglobulinemia | |||
|---|---|---|---|
| Feature | MGUS | Multiple Myeloma | Waldenström (WM) |
| Cell of origin | Plasma cell (benign) | Plasma cell (malignant) | Lymphoplasmacytic B-cell |
| M-protein | <3 g/dL, usually IgG | IgG > IgA > light chains | IgM (always) |
| BM infiltrate | Clonal plasma cells <10% | Clonal plasma cells ≥10% | Lymphoplasmacytic infiltrate |
| CRAB features | Absent | Present | Absent |
| Lytic bone lesions | No | Yes (skull, spine, ribs) | No |
| Hypercalcemia | No | Yes | No |
| Hyperviscosity | No | Rare | Yes (hallmark) |
| Lymphadenopathy / HSM | No | No | Yes |
| Progression | ~1%/year to MM | Malignant | Indolent lymphoma |
| Treatment | Observation | VRd ± ASCT | Plasmapheresis + rituximab-based |
Other look-alikes
- Metastatic bone disease (breast, prostate, lung) — lesions usually mixed / blastic, ALP elevated, bone scan positive.
- Primary hyperparathyroidism — hypercalcemia but PTH high, no M-protein or lytic lesions.
- Anemia of chronic / kidney disease — no M-spike, no lytic lesions.
| Important – فكرة سؤال | |
|
تذكر |
Management
MGUS & smoldering MM
- No treatment — active surveillance with SPEP + labs every 6–12 months to detect progression.
Multiple myeloma
Stratify by autologous stem-cell transplant (ASCT) eligibility.
- Induction (triplet VRd): bortezomib (proteasome inhibitor) 1.3 mg/m² SC + lenalidomide (immunomodulator) 25 mg PO daily on days 1–14 + dexamethasone 40 mg PO weekly. Anti-CD38 daratumumab is increasingly added up-front (quadruplet).
- ASCT — standard of care for fit patients <70 years.
- Maintenance: lenalidomide.
- Supportive care:
- Bisphosphonates — zoledronic acid 4 mg IV every 3–4 weeks (or pamidronate) for lytic disease and hypercalcemia.
- Radiotherapy — painful bone lesions, plasmacytomas, cord compression.
- Hydration + avoid nephrotoxins (NSAIDs, IV contrast); manage cast nephropathy.
- Vaccination (pneumococcal, influenza); VTE prophylaxis (aspirin 81 mg or LMWH — lenalidomide ↑ thrombosis risk).
Waldenström macroglobulinemia
- Plasmapheresis — urgent for symptomatic hyperviscosity (rapidly removes intravascular IgM).
- Rituximab-based chemoimmunotherapy or BTK inhibitors (ibrutinib).
Solitary plasmacytoma
- Local radiotherapy — often curative.
AL amyloidosis
- Anti-plasma-cell therapy as in MM (bortezomib-based ± daratumumab) to suppress the light-chain–producing clone.
Key Complications & Prognosis
Several complications are oncologic emergencies — recognise and treat immediately.
- Spinal cord compression (emergency) — vertebral lytic lesion / plasmacytoma. IV dexamethasone immediately + emergent MRI + radiotherapy or surgery.
- Hypercalcemia of malignancy — from osteoclast activation. IV isotonic fluids + calcitonin (rapid) + bisphosphonate (sustained) ± steroids.
- Myeloma kidney — light-chain cast nephropathy (± hypercalcemia, dehydration, NSAIDs, contrast). Hydrate, stop nephrotoxins, treat the clone.
- Recurrent infections — functional hypogammaglobulinemia → encapsulated organisms; a leading cause of death.
- Hyperviscosity syndrome — mainly WM (IgM); urgent plasmapheresis.
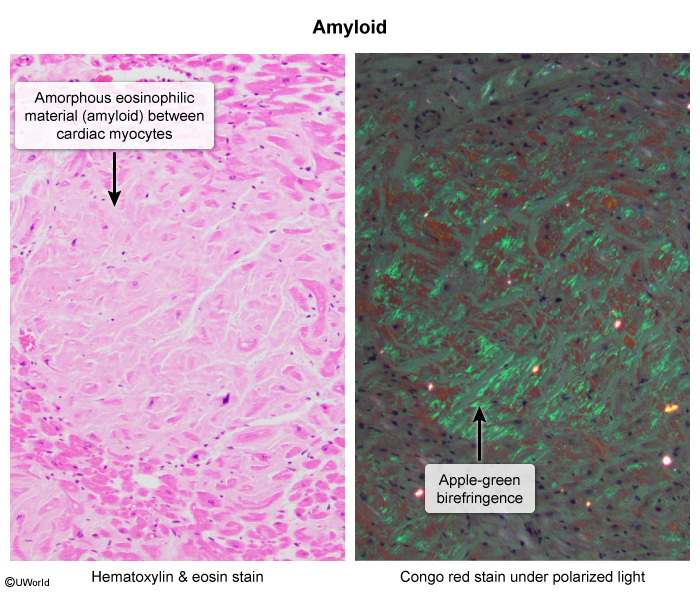
- AL amyloidosis — restrictive cardiomyopathy, nephrotic syndrome, macroglossia, periorbital purpura, neuropathy; biopsy shows apple-green birefringence on Congo red under polarized light.
- Venous thromboembolism (VTE) — disease + lenalidomide; aspirin or LMWH prophylaxis.
(تنبيه: انضغاط الحبل الشوكي حالة طارئة في الأورام — ابدأ الديكساميثازون وريدياً فوراً قبل تأكيد التشخيص بالرنين المغناطيسي).
Prognosis
- MM is staged by the R-ISS using β2-microglobulin, albumin, LDH, and high-risk cytogenetics (e.g., t(4;14), del(17p)).
- MGUS progresses ~1%/year and smoldering MM ~10%/year to overt MM.
- MM remains incurable, but novel agents + ASCT have markedly improved median survival; infection and renal failure are the leading causes of death.
The Complications of Multiple Myeloma lays out each complication alongside its management, and the AL vs AA amyloidosis comparison separates plasma-cell–derived amyloid from inflammatory amyloid.
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.