شرح المدرسين

Summary
Leukemias are malignant clonal proliferations of hematopoietic stem cells in the bone marrow categorized by onset and lineage into four primary entities: AML (adults, myeloblasts, Auer rods, MPO-positive), ALL (children, lymphoblasts, TdT-positive), CML (middle-aged, mature granulocytes, t(9;22) BCR-ABL, low LAP score), and CLL (elderly, mature B-cells, CD5+/CD19+, smudge cells). Acute leukemias present rapidly with bone marrow failure defined by >= 20% blasts, requiring bone marrow biopsy and flow cytometry for gold-standard diagnosis. Urgent management principles include all-trans retinoic acid (ATRA) for APL-associated DIC, tyrosine kinase inhibitors (imatinib) for CML, intrathecal chemotherapy for ALL CNS prophylaxis, and aggressive hydration with allopurinol or rasburicase to prevent tumor lysis syndrome.
Overview
Leukemias are malignant clonal proliferations of white-cell precursors arising in the bone marrow. A single hematopoietic stem/progenitor cell acquires a driver mutation, proliferates uncontrollably, and crowds out normal hematopoiesis → marrow failure + circulating abnormal cells.
Two classification axes
- Speed / maturity → Acute (immature blasts ≥ 20% of marrow; rapid, marrow failure in weeks) vs Chronic (relatively mature cells; indolent, often found incidentally on a routine CBC).
- Lineage → Myeloid vs Lymphoid.
Crossing these two axes yields the four classic leukemias:
| The 2×2 Classification of Leukemia | ||
|---|---|---|
| Onset \ Lineage | Myeloid | Lymphoid |
| Acute (blasts ≥ 20%) | AML — adults (~65 y) | ALL — children (2–5 y) |
| Chronic (mature cells) | CML — middle-aged (45–55 y) | CLL — elderly (> 60 y) |
(ملاحظة سريرية: عتبة الـ 20% من الأرومات (blasts) في نقي العظم أو الدم المحيطي هي الحد الفاصل الذي يُعرّف اللوكيميا الحادة عن المزمنة.)
| Leukemia age groups — «ALL CALM» | |
| ALL → kids (Children, 2–5 y) AML → Adults (~65 y) CML → Middle-aged (45–55 y) CLL → Late adulthood / elderly (> 60 y) |
جملة تذكرية |
Diagnostic Principles
Shared clinical features (any leukemia)
All four converge on the consequences of marrow replacement plus tissue infiltration:
- Anemia → fatigue, pallor, dyspnea.
- Thrombocytopenia → petechiae, easy bruising, mucosal bleeding.
- Neutropenia / dysfunctional WBCs → recurrent infections, fever.
- Organ infiltration → hepatosplenomegaly, lymphadenopathy, bone pain.
Universal diagnostic workup
The same stepwise workup applies to any suspected leukemia:
- CBC + peripheral smear → WBC count, and morphologic clues: blasts, Auer rods, smudge cells, basophilia.
- Bone marrow aspiration & biopsy → confirms diagnosis; ≥ 20% blasts = acute leukemia.
- Flow cytometry / immunophenotyping → assigns lineage (myeloid vs lymphoid; B vs T).
- Cytogenetics / FISH / PCR → translocations drive prognosis & therapy:
- t(9;22) BCR-ABL → CML and Ph⁺ ALL.
- t(15;17) PML-RARα → APL.
- t(12;21) → favorable pediatric ALL; t(8;21)/inv(16) → favorable AML.
- LDH, uric acid, K⁺, phosphate, Ca²⁺, creatinine → baseline tumor-lysis risk.
- Lumbar puncture → for ALL (CNS staging) or any CNS symptoms.
Quick smear pearls
- Auer rods → AML (especially APL).
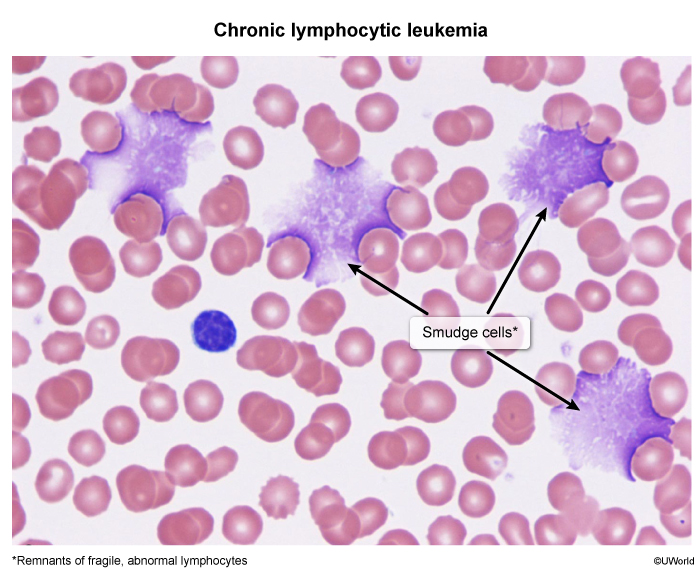
- Smudge cells → CLL.
- Full myeloid spectrum + basophilia → CML.
- TdT-positive blasts → ALL.
Acute Leukemias: ALL vs. AML
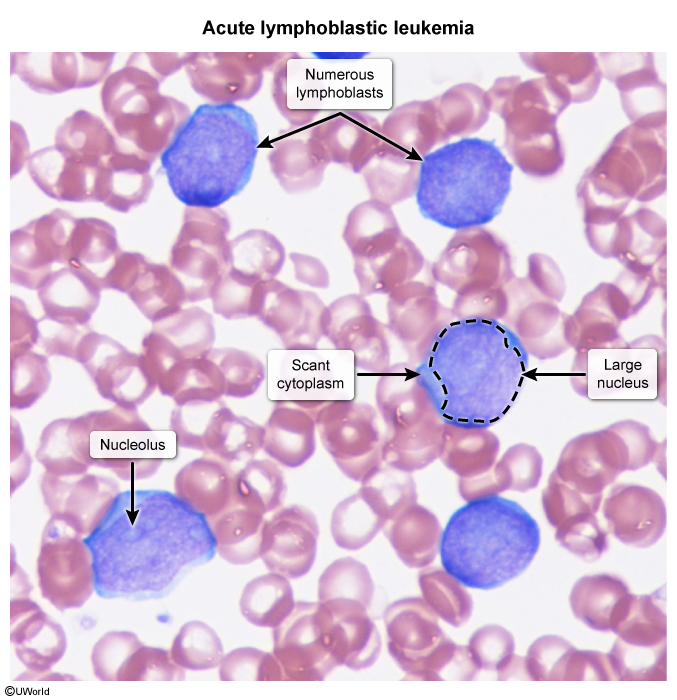
Both are defined by ≥ 20% blasts and an aggressive course, but they split cleanly by age and lineage: ALL = lymphoid blasts in children; AML = myeloid blasts in adults.
Epidemiology & risk factors
- ALL — most common childhood malignancy; peak 2–5 years; B-cell ≫ T-cell. Strongly associated with Down syndrome.
- AML — most common acute leukemia in adults (median ~65 y). Risk factors: prior chemotherapy (alkylating agents, topoisomerase-II inhibitors), radiation, benzene, smoking, transformation from MDS/myeloproliferative disorders, and Down syndrome (especially AML M7, megakaryoblastic, in children < 5 y).
Clinical clues
- ALL: marrow failure + bone pain / limp, lymphadenopathy, hepatosplenomegaly, CNS involvement (headache, cranial-nerve palsies). T-ALL → anterior mediastinal mass in a teenage boy (may cause SVC syndrome). Testes = sanctuary site and common relapse location.
- AML: marrow failure + leukostasis (WBC > 50–100k → headache, dyspnea, visual changes, priapism), gum hypertrophy and leukemia cutis (monocytic subtypes M4/M5), and DIC at presentation in APL (M3).
Diagnosis & morphology
Both show marrow blasts ≥ 20%; the lineage is settled by morphology and flow cytometry:
- ALL: small blasts, scant cytoplasm, NO Auer rods; TdT-positive is the hallmark (ملاحظة سريرية: إنزيم الـ TdT النووي هو السمة المميزة للأرومات اللمفاوية ويغيب في اللوكيميا النقوية). B-ALL → CD10/CD19/CD20; T-ALL → CD2–CD8. Cytogenetics: t(12;21) = good (children); t(9;22) Philadelphia = poor.
- AML: Auer rods + myeloperoxidase (MPO)-positive blasts; flow CD13/CD33/CD117. Auer rods are myeloid-specific (ملاحظة سريرية: قضبان أوير (Auer rods) نوعية للنسيلة النقوية وتؤكد تشخيص AML وتستبعد ALL). Key cytogenetics: t(15;17) PML-RARα → APL (M3); t(8;21)/inv(16) → favorable.
See the ALL epidemiology, clinical features, and diagnosis reference for the full pediatric workup including CNS staging.
Treatment
- ALL: multi-phase chemotherapy — induction → consolidation → maintenance (~2–3 years total) + intrathecal methotrexate for CNS prophylaxis (mandatory). Add a TKI (imatinib) if Ph⁺. Childhood cure ~90%; adults do worse.
- AML: «7 + 3» induction — cytarabine × 7 days + an anthracycline × 3 days. APL exception: ATRA + arsenic trioxide (best-prognosis AML). Allogeneic stem cell transplant for high-risk or relapsed disease.
| Acute leukemia buzzwords | |
| Auer rods = AML (especially M3/APL); MPO-positive blasts. TdT⁺ blasts = ALL (lymphoid lineage). t(15;17) → APL → give ATRA («15 + 17 → ATRA»). Child + bone pain ± anterior mediastinal mass → think T-ALL. |
جملة تذكرية |
Chronic Leukemias: CML vs. CLL
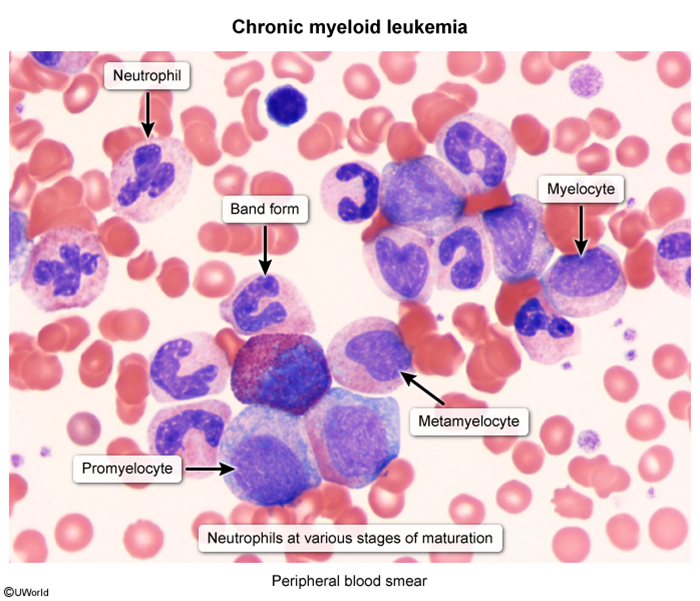
Both are indolent, frequently asymptomatic, and often discovered on a routine CBC. They diverge by lineage: CML is a myeloproliferative neoplasm of mature granulocytes; CLL is an accumulation of mature but incompetent B-lymphocytes.
Pathogenesis & epidemiology
- CML — driven by the Philadelphia chromosome → t(9;22) → BCR-ABL fusion → constitutively active tyrosine kinase (ملاحظة سريرية: انتقال t(9;22) المنتج لجين BCR-ABL هو السمة الجزيئية المُعرِّفة لـ CML وهدف العلاج الموجَّه). Median age ~45–55 y.
- CLL — monoclonal proliferation of mature B-cells; most common adult leukemia in the West; age usually > 60 y. Considered the same disease as small lymphocytic lymphoma (SLL).
Clinical clues
- CML: massive splenomegaly (LUQ fullness, early satiety), fatigue, night sweats, weight loss; hyperviscosity if WBC very high.
- CLL: painless lymphadenopathy, hepatosplenomegaly, B symptoms when advanced; recurrent infections from hypogammaglobulinemia; autoimmune cytopenias — warm AIHA (Coombs⁺) and ITP.
CML — three phases
- Chronic phase (~85% at diagnosis) → high WBC, < 10% blasts.
- Accelerated phase → 10–19% blasts, worsening symptoms.
- Blast crisis → ≥ 20% blasts; behaves like acute leukemia (≈2/3 myeloid, 1/3 lymphoid).
The clinical phases of CML by blast percentage lay out how the disease escalates from stable chronic phase to blast crisis.
Diagnosis & morphology
- CML: WBC often > 100,000 with all stages of granulocyte maturation, plus basophilia & eosinophilia. LAP score is LOW (ملاحظة سريرية: انخفاض إنزيم الفوسفاتاز القلوي للكريات البيض (LAP) هو السمة المميزة التي تفرق CML عن التفاعل الابيضاضي الشديد). Confirm with BCR-ABL by FISH/PCR or cytogenetic t(9;22).
- CLL: absolute B-lymphocyte count ≥ 5,000/µL of clonal, mature-appearing cells; smudge cells on smear (fragile lymphocytes crushed during slide prep) (ملاحظة سريرية: خلايا اللطخة (smudge cells) ناتجة عن هشاشة اللمفاويات وتُعدّ مؤشراً مميزاً لـ CLL). Flow cytometry: CD5⁺, CD19⁺, CD20⁺, CD23⁺ (CD5 = a T-cell marker aberrantly expressed on these B-cells).
Refer to the CLL diagnostic criteria and treatment indications for the flow-cytometry panel and the thresholds that trigger therapy.
Treatment
- CML: Imatinib (or dasatinib/nilotinib) — first-line TKI with excellent response; allogeneic stem cell transplant reserved for TKI failure or blast crisis.
- CLL: Early/asymptomatic → watchful waiting (no survival benefit from early treatment). Symptomatic/advanced → BTK inhibitor (ibrutinib), BCL-2 inhibitor (venetoclax), or anti-CD20 (rituximab) ± chemo (FCR).
Disease-specific complication
- CLL → Richter transformation: evolution to diffuse large B-cell lymphoma (DLBCL) — rapidly enlarging node, new B symptoms, aggressive course and poor prognosis.
- CML → blast crisis: transformation to acute leukemia.
| Important – فكرة سؤال | |
|
CD5 is normally a T-cell antigen, yet it is aberrantly co-expressed (with CD19/CD20/CD23) on the malignant B-cells of CLL. The other classic CD5⁺ B-cell neoplasm is mantle cell lymphoma — separate them: mantle cell is CD23-negative with t(11;14) / cyclin D1 overexpression, whereas CLL is CD23-positive. |
تذكر |
| Chronic leukemia buzzwords | |
| Philadelphia = CML → «9 on top of 22» → t(9;22) → BCR-ABL. ↓ LAP score = CML (↑ LAP in leukemoid reaction). Smudge cells = CLL → «CLL crushes its cells». Massive splenomegaly + basophilia → CML. |
جملة تذكرية |
Master Comparison & Key Differentials
This is the must-memorize backbone of the topic — the single matrix that most exam questions test one row of. Read it across (one disease) and down (one feature) until each cell is automatic.
| Side-by-Side Comparison: ALL vs AML vs CML vs CLL | ||||
|---|---|---|---|---|
| Feature | ALL | AML | CML | CLL |
| Typical age | Children (2–5 y) | Adults (~65 y) | Middle-aged (45–55 y) | Elderly (> 60 y) |
| Cell type | Lymphoblasts (mostly B) | Myeloblasts | Mature myeloid spectrum | Mature B-lymphocytes |
| Key marker | TdT⁺, CD10/CD19 | MPO⁺, Auer rods, CD13/CD33/CD117 | BCR-ABL / t(9;22) | CD5⁺, CD19/CD20/CD23⁺ |
| Smear clue | Blasts, NO Auer rods | Auer rods; APL → DIC | Full myeloid spectrum, basophilia, ↓ LAP | Smudge cells |
| Cytogenetics | t(12;21) favorable; t(9;22) poor | t(15;17) → APL; t(8;21)/inv(16) favorable | t(9;22) BCR-ABL | del(13q), del(11q), del(17p) |
| Special association | Down syndrome; CNS & testicular spread | Down syndrome, prior chemo/radiation, MDS | Massive splenomegaly; blast crisis | Warm AIHA, ITP, hypogammaglobulinemia, Richter |
| First-line Tx | Multi-agent chemo + IT methotrexate | «7 + 3»; ATRA + arsenic for APL | Imatinib (TKI) | Watchful waiting; ibrutinib if symptomatic |
| Prognosis | Children ~90% cure | Variable; APL best | Excellent on TKIs | Indolent; Richter = aggressive |
Key differential: CML vs leukemoid reaction
A reactive neutrophilia (severe infection, sepsis) can mimic CML on the smear. The decisive separators are the LAP score, BCR-ABL, and basophilia (ملاحظة سريرية: ارتفاع الـ LAP مع غياب BCR-ABL يرجّح التفاعل الابيضاضي، بينما انخفاض الـ LAP مع وجود BCR-ABL يؤكد CML).
| CML vs Leukemoid Reaction | ||
|---|---|---|
| Feature | CML | Leukemoid reaction |
| LAP (leukocyte alkaline phosphatase) score | LOW (↓) | HIGH (↑) |
| BCR-ABL / t(9;22) | Present | Absent |
| Basophilia | Present (absolute basophilia) | Absent |
| Underlying cause | Clonal myeloproliferative neoplasm | Reactive (severe infection, sepsis, inflammation) |
| Toxic granulation / Döhle bodies | Absent | Present |
| Splenomegaly | Massive | Mild or absent |
See the library's leukemoid reaction vs CML comparison for the same differential framed around the low-vs-high LAP score and BCR-ABL status.
Urgent Complications
Beyond marrow failure, three time-critical emergencies dominate exam questions and must be recognized on sight: tumor lysis syndrome, leukostasis, and APL-associated DIC.
1. Tumor Lysis Syndrome (TLS)
- Mechanism: massive tumor cell death (spontaneous or with chemotherapy) dumps intracellular contents into the blood.
- Metabolic tetrad: ↑ K⁺, ↑ phosphate, ↑ uric acid, ↓ Ca²⁺ (calcium falls as it binds the released phosphate) → AKI, arrhythmias, tetany/seizures.
- Highest risk: ALL, Burkitt lymphoma, AML with high WBC / bulky, rapidly proliferating disease.
- Prevention: aggressive IV hydration + allopurinol (xanthine oxidase inhibitor) for standard risk; rasburicase for high risk.
The tumor lysis syndrome risk stratification and prophylaxis lays out the high/intermediate/low risk categories and the rasburicase-vs-allopurinol decision.
| Important – فكرة سؤال | |
|
Rasburicase (recombinant urate oxidase) is contraindicated in G6PD deficiency — it generates hydrogen peroxide as it degrades uric acid, precipitating severe hemolysis and methemoglobinemia. In G6PD-deficient patients at risk of tumor lysis syndrome, use allopurinol + aggressive IV hydration instead. |
تذكر |
2. Leukostasis
- Trigger: WBC > 50,000–100,000 — typically AML or blast-crisis CML.
- Mechanism: sludging of bulky blasts in the microvasculature → tissue hypoxia.
- Features: dyspnea, headache, blurred vision, altered mental status, priapism.
- Emergency management: leukapheresis + hydroxyurea + prompt induction chemotherapy.
3. APL-associated DIC
- Acute promyelocytic leukemia (AML M3, t(15;17)) presents with disseminated intravascular coagulation — the malignant promyelocytes release procoagulant granules.
- Bleeding can be fatal before treatment even begins (ملاحظة سريرية: التخثر المنتشر داخل الأوعية (DIC) في APL هو حالة إسعافية؛ يجب البدء بالـ ATRA فور الاشتباه السريري قبل تأكيد الوراثيات الخلوية).
- Smear: abnormal promyelocytes with abundant cytoplasm and bundles of Auer rods.
| Important – فكرة سؤال | |
|
In suspected APL (AML M3) — promyelocytes packed with bundles of Auer rods, t(15;17), and DIC at presentation — start ATRA (all-trans retinoic acid) IMMEDIATELY on clinical suspicion, before cytogenetic confirmation returns. ATRA differentiates the malignant promyelocytes and rapidly reverses the lethal coagulopathy; delaying therapy to await confirmation can be fatal from hemorrhage. |
تذكر |
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.