Summary
Anemia of chronic disease (ACD), or anemia of inflammation, is a mild-to-moderate, typically normocytic normochromic anemia (MCV 80–100 fL, occasionally microcytic in long-standing disease) driven by sustained immune activation. Its core mechanism is hepcidin-mediated iron sequestration: inflammatory cytokines (primarily IL-6) stimulate hepatic production of hepcidin, which degrades ferroportin on enterocytes and reticuloendothelial macrophages, trapping body iron in stores and blunting the erythropoietin (EPO) response. Associated etiologies include chronic infections, autoimmune conditions, malignancies, and chronic kidney disease (CKD). Peripheral blood smear typically reveals normal erythrocyte morphology. Diagnostic findings feature low serum iron, low TIBC, and elevated serum ferritin (an acute-phase reactant). Primary treatment focuses on resolving the underlying disease; routine oral iron is ineffective due to hepcidin-blocked gut absorption, though IV iron or erythropoiesis-stimulating agents (ESAs) may be used in specific cases like CKD.
Overview
Anemia of chronic disease (ACD), also called anemia of inflammation, is a mild-to-moderate anemia that develops in patients with sustained immune activation (chronic infection, autoimmune disease, malignancy, or CKD). It is the second most common anemia worldwide after iron deficiency.
- Typical picture: mild normocytic, normochromic anemia (MCV 80–100) in a patient with a known chronic illness.
- Can drift to microcytic, hypochromic only if long-standing/severe.
- Hb rarely falls below 8 g/dL on ACD alone — if it does, hunt for a second cause (bleeding, hemolysis, marrow infiltration).
The core lesion is a functional iron deficiency: body iron stores are normal or increased, but the iron is "locked away" and cannot reach the marrow for erythropoiesis.
Pathophysiology
The inflammation → IL-6 → hepcidin axis
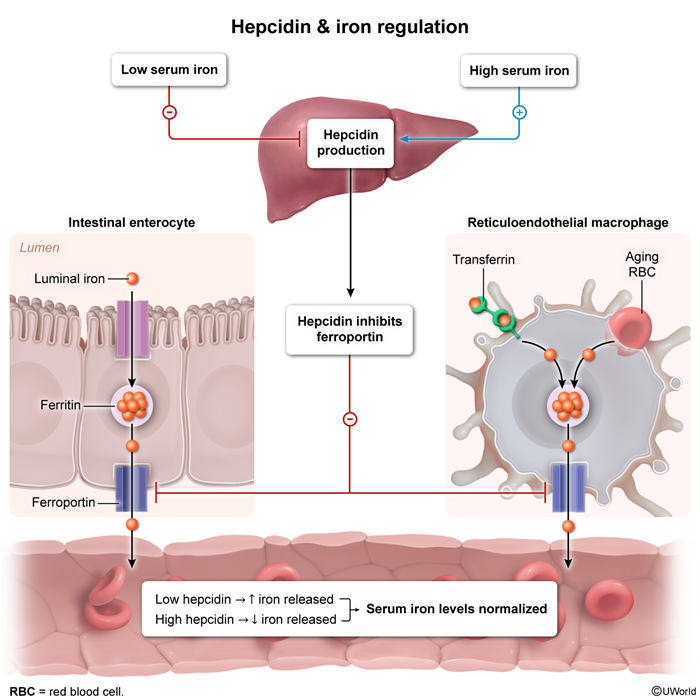
Chronic inflammation drives release of IL-6 (and other cytokines), which signals the liver to make hepcidin — the master regulator of iron. Hepcidin produces three downstream effects:
- Iron sequestration: hepcidin degrades ferroportin on macrophages → iron is trapped in the reticuloendothelial system → ↑ ferritin (storage form rises).
- ↓ Gut absorption: hepcidin degrades ferroportin on duodenal enterocytes → less dietary iron enters the blood.
- ↓ Erythropoiesis: cytokines (IL-1, TNF-α, IFN-γ) blunt the marrow's response to EPO and shorten RBC lifespan.
Net effect: iron is present but unavailable → the marrow cannot make enough hemoglobin → mild anemia. Teleologically, this iron lockdown evolved to starve bacteria of iron during infection — the anemia is a side effect of that defense.
| Mnemonic – Hepcidin Hides Iron | |
|
"Hepcidin Hides Iron"
The body's "iron-lockdown hormone" during inflammation — meant to starve bacteria of iron, but ends up starving the marrow too. |
جملة تذكرية |
Etiology
Any disease producing sustained inflammation can cause ACD. The four classic categories — remember "CIA-K":
| Mnemonic – Causes of ACD | |
"CIA-K" = the 4 categories of ACD:
|
جملة تذكرية |
| The 4 Classic Categories of ACD | |
| 1 | Chronic infections |
| Tuberculosis | Classic exam association |
| Osteomyelitis / endocarditis | Chronic bacterial infection |
| 2 | Autoimmune disease |
| Rheumatoid arthritis | Most common autoimmune cause |
| SLE / IBD | Lupus, Crohn, ulcerative colitis |
| 3 | Malignancy |
| Solid tumors | Lung, breast, colon |
| Hematologic | Lymphoma, multiple myeloma |
| 4 | Chronic kidney disease |
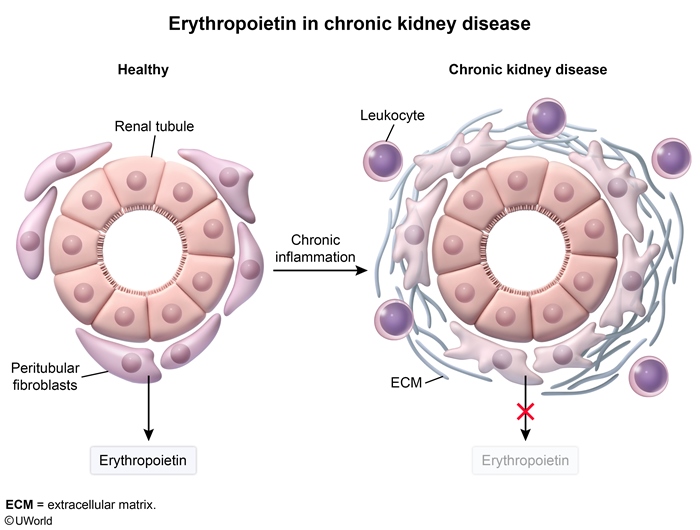
| ↓ Erythropoietin | Failing kidney → no EPO |
| ↑ Hepcidin | Uremia + inflammation |
Special note on CKD: anemia of CKD overlaps with ACD but adds a second mechanism — the damaged kidney makes less erythropoietin. This is why CKD anemia responds to EPO injections while pure ACD usually does not.
Clinical Presentation
ACD is usually mild and well-tolerated; the anemia itself is frequently asymptomatic and overshadowed by the underlying disease.
- Nonspecific anemia symptoms: fatigue, weakness, pallor, mild exertional dyspnea.
- Onset: gradual over weeks to months after the chronic disease becomes active.
- Severity: Hb usually 9–11 g/dL; Hb < 8 g/dL is unusual — search for a second cause.
Features of the underlying disease dominate the picture:
- Joint pain/stiffness → RA; butterfly rash → SLE.
- Fever, night sweats, weight loss → TB or malignancy.
- Uremic symptoms → CKD.
There are no physical signs specific to ACD. The diagnosis is made by combining a known chronic illness + a characteristic lab pattern (covered next).
| Important – فكرة سؤال | |
A patient with rheumatoid arthritis on long-term therapy presents with fatigue. CBC shows mild normocytic anemia. Which iron-study pattern do you expect? Answer: ↓ serum iron, ↓ TIBC, ↑ ferritin, normal/↓ transferrin saturation. The low TIBC and high ferritin are the two findings that separate ACD from iron deficiency anemia (where TIBC is high and ferritin is low). |
تذكر |
Diagnostic Approach
ACD is a laboratory diagnosis in a patient with a known chronic disease — there is no single confirmatory test. Build the picture from three blocks of results.
1. CBC
- Mild anemia, Hb 9–11 g/dL.
- MCV usually normal; may become low only in chronic, severe disease.
- Reticulocyte count low or inappropriately normal — the marrow is hypoproliferative.
2. Iron studies — the key step
- Serum iron: ↓ Low
- TIBC (transferrin): ↓ Low
- Ferritin (stores): ↑ High (or normal)
- Transferrin saturation: normal or ↓
3. Inflammatory markers
- ↑ ESR and ↑ CRP support the diagnosis but are non-specific.
- Ferritin is itself an acute-phase reactant — which is exactly why it rises in ACD.
The single highest-yield exam skill is distinguishing ACD from its mimics. Use the master table below; for an external cross-check, see the Iron Studies in Microcytic Anemia comparison table for the ferritin/TIBC/transferrin-saturation pattern across all three conditions.
| Master Table – ACD vs Iron Deficiency vs Thalassemia Minor | |||
|---|---|---|---|
| Parameter | ACD | Iron deficiency anemia | Thalassemia minor |
| MCV | Normal (later ↓ low) | ↓ Low | ↓↓ Very low (often <70) |
| RBC count | Low | Low | Normal / high |
| Serum iron | ↓ Low | ↓ Low | Normal |
| TIBC (transferrin) | ↓ Low | ↑ High | Normal |
| Ferritin (stores) | ↑ High / normal | ↓ Low | Normal |
| Transferrin saturation | Normal / ↓ | ↓↓ Very low | Normal |
| RDW | Normal | ↑ High | Normal |
| Key extra clue | ↑ ESR/CRP; iron trapped in macrophages | Absent marrow iron | ↑ HbA2 (β-thal) on electrophoresis |
| فخ امتحاني – Exam Trap | |
أهم ما يميز فقر دم الأمراض المزمنة عن نقص الحديد هو ارتفاع الفيريتين (مخزون الحديد) وانخفاض الـ TIBC. في نقص الحديد، يحدث العكس تماماً. |
ملاحظة |
| Mnemonic – ACD iron studies | |
"ACD = All Down except Ferritin"
In IDA it is the mirror image: ferritin goes DOWN and TIBC goes UP. |
جملة تذكرية |
On the peripheral smear, ACD typically shows  normocytic normochromic cells, becoming microcytic/hypochromic only in advanced disease.
normocytic normochromic cells, becoming microcytic/hypochromic only in advanced disease.
| Note – ملاحظة | |
The tricky case is coexisting ACD + IDA (e.g., RA patient with NSAID-induced GI bleed). Ferritin may be falsely "normal."
|
ملاحظة |
Management
Management is built around four numbered priorities. The anemia improves as inflammation subsides, so the underlying disease is always the main target.
- Treat the underlying disease (the definitive fix):
- Antibiotics for chronic infection (TB, osteomyelitis).
- DMARDs/immunosuppressants for RA, SLE, IBD.
- Chemotherapy for malignancy; dialysis/renal optimization for CKD.
- Iron therapy — only if true iron deficiency coexists:
- Do not give oral iron routinely — hepcidin blocks gut absorption, so it fails.
- If iron deficiency is genuinely present (low ferritin, transferrin saturation < 20%), give IV iron (bypasses the gut).
- Erythropoiesis-stimulating agents (ESAs):
- Indicated mainly for anemia of CKD and selected chemotherapy-induced ACD.
- Target Hb 10–11 g/dL — higher targets raise thrombosis, stroke, and death risk.
- ESA resistance: if no response, look for causes of ESA resistance — iron deficiency, ongoing inflammation, or vitamin deficiency.
- Transfusion:
- Reserved for severe symptomatic anemia (Hb < 7–8 g/dL) or acute decompensation.
- Not a long-term solution.
Key complications
- Cardiovascular stress: in the elderly or those with heart disease, even mild anemia can worsen angina or heart failure.
- Masked coexisting iron deficiency: ACD can hide a GI bleed (classic RA-on-NSAIDs exam trap) — reduced quality of life and impaired wound healing follow.
- ESA-related thrombosis: EPO therapy can cause hypertension, thromboembolic events, and increased mortality if Hb is pushed above 11–12 g/dL.
| ملاحظة مهمة – Management Pearl | |
في فقر دم الأمراض المزمنة (ACD) لا تعطِ حديد عن طريق الفم بشكل روتيني — الهبسيدين يمنع امتصاصه من الأمعاء. إذا وُجد نقص حديد حقيقي مصاحب (ferritin منخفض)، يُفضّل الحديد عن طريق الوريد. علاج المرض الأساسي هو الحل الجذري. |
ملاحظة |
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.