شرح المدرسين

Summary
Iron deficiency anemia (IDA) is the leading cause of microcytic hypochromic anemia (MCV < 80 fL), resulting from depleted total body iron and impaired heme synthesis. Etiologies include chronic blood loss (GI malignancy in men/postmenopausal women; menorrhagia in premenopausal women), malabsorption (celiac disease), and increased demand (pregnancy). Pathophysiology follows sequential depletion: serum ferritin drops first (most specific marker), followed by decreased serum iron and elevated TIBC, with microcytic anemia appearing last.
Clinical hallmarks include fatigue, pica (ice craving), koilonychia, angular cheilitis, and pencil cells with an elevated RDW on peripheral smear.
Diagnosis requires iron studies (low ferritin, low transferrin saturation, high TIBC); an endoscopic GI workup is mandatory in adults to rule out bleeding. Treatment centers on oral ferrous sulfate (administered with vitamin C) or IV iron if oral therapy fails, alongside addressing the underlying cause.
Overview
Iron deficiency anemia (IDA) is the most common anemia worldwide and the leading cause of microcytic hypochromic anemia (MCV <80 fL). It results from depleted total body iron, leading to insufficient heme synthesis. Iron deficiency can exist without anemia (latent stage) — ferritin drops before Hb falls.
- Anemia thresholds: Hb <13 g/dL (men), <12 g/dL (non-pregnant women), <11 g/dL (pregnancy/children).
- High-risk groups: women of reproductive age, pregnant women, infants 6 mo–2 yr, adolescents, elderly with chronic GI blood loss.
Etiology — most tested causes
Think: where is the iron going, or why isn't it coming in?
- Chronic blood loss (most common in adults):
- GI bleeding — colon cancer, peptic ulcer disease, NSAID/aspirin use, hookworm → most common cause in adult men & postmenopausal women
- Menorrhagia → most common cause in premenopausal women
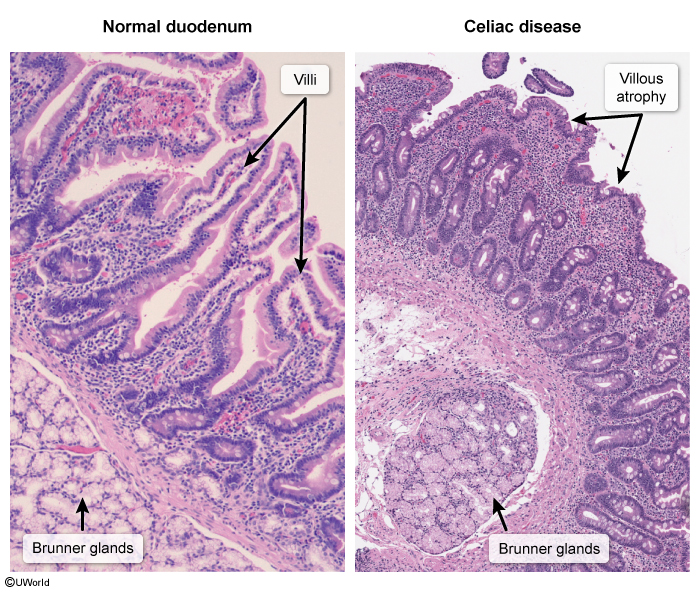
- Malabsorption: celiac disease (duodenal villous atrophy), post-gastrectomy/bariatric surgery, H. pylori, chronic PPI use
- Increased demand: pregnancy (fetal demand + expanded blood volume), infancy/adolescence (rapid growth)
- Decreased intake: exclusive breastfeeding without supplementation, excess cow's milk (<1 yr), strict vegan diet
| Mnemonic – Causes of IDA: "Bleeding, Lack, Loss, Load" | |
| Bleeding (GI, menstrual) — most common in adults Lack of intake (diet — infants on cow's milk, vegans) Loss of absorption (celiac, gastrectomy, PPIs) Load / demand (pregnancy, growth spurts) |
جملة تذكرية |
Pathophysiology
Pathophysiology
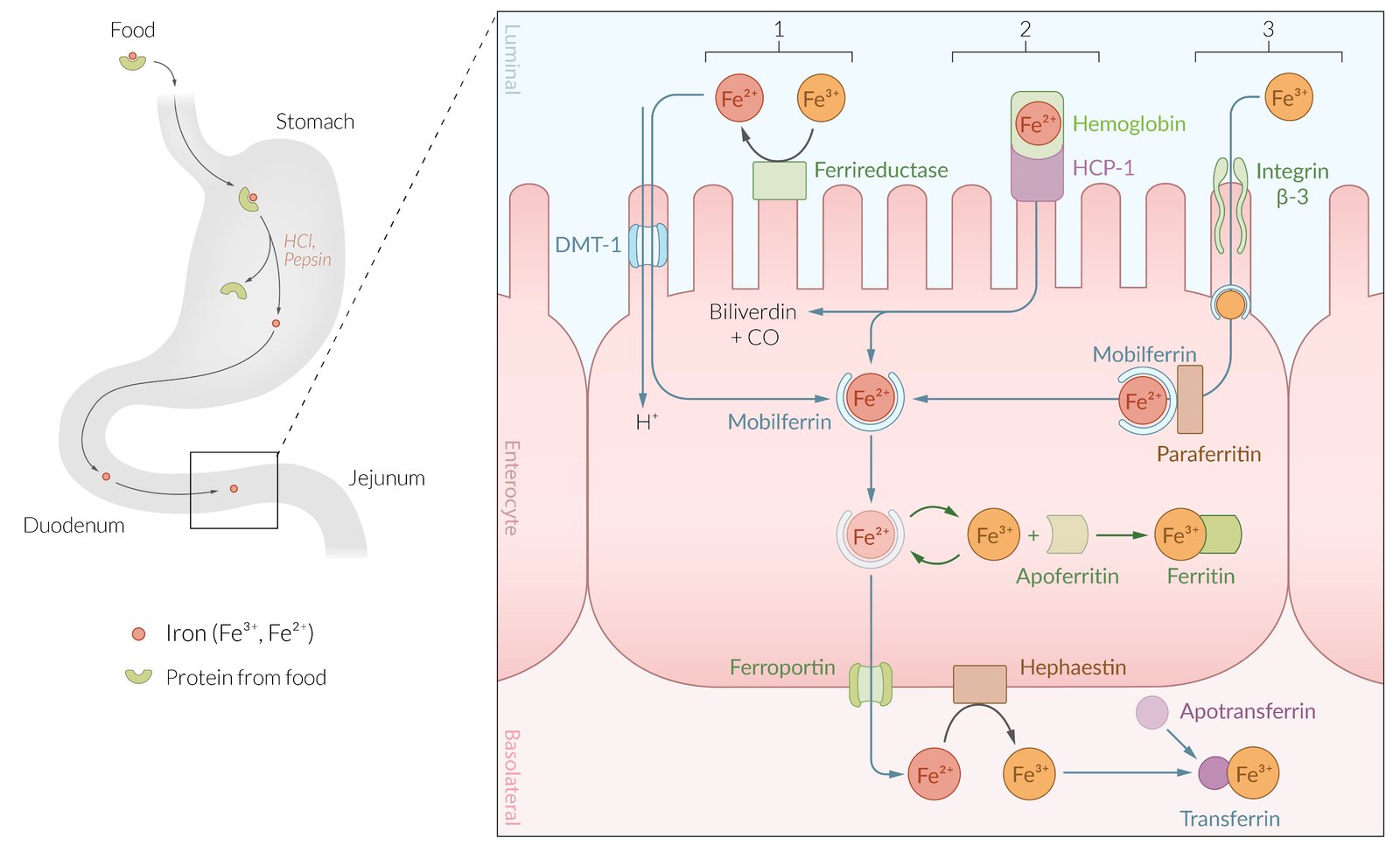
Dietary iron (heme > non-heme) is absorbed in the duodenum. Gastric acid converts Fe³⁺ → Fe²⁺ for absorption via DMT1. Inside enterocytes, iron is stored as ferritin or exported via ferroportin into blood, where it binds transferrin for delivery to bone marrow. Hepcidin (the master regulator, from the liver) degrades ferroportin — when body iron is low, hepcidin falls, allowing more absorption.
Sequence of depletion in IDA:
- Stage 1 — Storage iron ↓: ferritin drops first (earliest marker); Hb and MCV still normal.
- Stage 2 — Transport iron ↓: serum iron ↓, TIBC ↑ (body builds more "transport trucks"), transferrin saturation ↓.
- Stage 3 — Functional iron ↓: heme synthesis fails → RBCs released microcytic (small) and hypochromic (pale) → Hb falls → anemia appears last.
| Mnemonic – Stages of Iron Deficiency: "Store → Transport → Cell" | |
| Iron depletes in this order: 1. Storage iron ↓ → ferritin falls first (earliest marker) 2. Transport iron ↓ → serum iron ↓, TIBC ↑, transferrin saturation ↓ 3. Functional (cellular) iron ↓ → Hb falls, MCV falls → anemia appears last |
جملة تذكرية |
Clinical Presentation
General anemia symptoms (non-specific)
- Fatigue, weakness, decreased exercise tolerance
- Pallor (conjunctiva, palmar creases, nail beds)
- Dyspnea on exertion, tachycardia, palpitations
- Headache, dizziness, syncope
IDA-specific findings (high-yield exam buzzwords)
- Pica — craving non-food items: ice (pagophagia), dirt, clay, starch
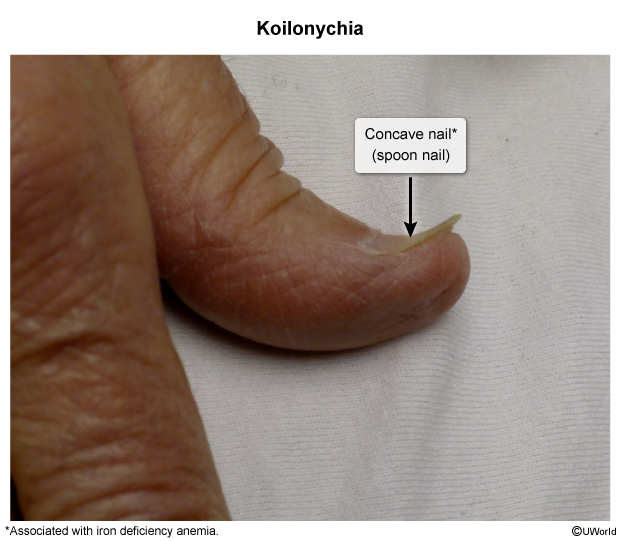
- Koilonychia — spoon-shaped, brittle nails
- Angular cheilitis — fissures at corners of the mouth
- Atrophic glossitis — smooth, beefy red tongue
- Restless legs syndrome
- Plummer–Vinson syndrome (rare): IDA + esophageal web + dysphagia → ↑ risk of esophageal squamous cell carcinoma
Pediatric features
- Irritability, poor school performance, developmental delay (may be irreversible if prolonged)
- Breath-holding spells — IDA is a recognized risk factor; see the Breath-Holding Spells: Risk Factors, Clinical Features, Evaluation, and Treatment for the full association.
- Classic scenario: toddler drinking excessive cow's milk (>24 oz/day), refusing solids
Peripheral blood smear
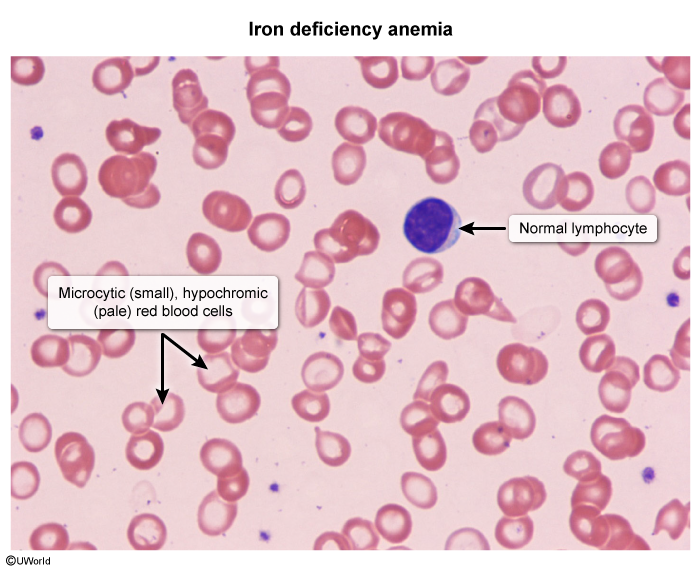
Microcytic, hypochromic RBCs with marked central pallor, anisocytosis (varying sizes reflecting ↑RDW), poikilocytosis, and characteristic pencil (cigar) cells.
Diagnostic Approach
Step 1 — CBC
- ↓ Hb, ↓ MCV (<80 fL), ↓ MCH/MCHC (hypochromic)
- ↑ RDW — often the earliest CBC clue (mixed cell sizes from ongoing deficient erythropoiesis)
- Reticulocyte count: low or inappropriately normal (production defect)
Step 2 — Iron studies (confirm the diagnosis)
| Test | Result in IDA | Clinical significance |
|---|---|---|
| Ferritin | ↓↓ (<15 ng/mL diagnostic; <30 highly suggestive) | Reflects depleted stores — most specific single test |
| Serum iron | ↓ | Less iron in circulation |
| TIBC / transferrin | ↑ | Liver upregulates transferrin to scavenge iron |
| Transferrin saturation | ↓ (<15%) | Less iron bound to more transferrin |
| Important – فكرة سؤال | |
| Ferritin is an acute-phase reactant. In patients with concurrent infection, malignancy, or inflammation, ferritin may be falsely normal or elevated despite true iron deficiency. When suspicion is strong, check transferrin saturation or soluble transferrin receptor (sTfR) — sTfR is ↑ in IDA but normal in anemia of chronic disease. | تذكر |
| فخ امتحاني – Exam Trap | |
| قد يكون مستوى الفيريتين طبيعياً أو مرتفعاً بشكل كاذب في حالات الالتهاب، مما يخفي نقص الحديد الحقيقي. استخدم مستوى تشبع الترانسفيرين أو مستقبل الترانسفيرين الذائب (sTfR) للتأكد. | ملاحظة |
Step 3 — Differentiate from other microcytic anemias
All microcytic anemias look similar on CBC — iron studies separate them. Remember TICS: Thalassemia, Iron deficiency, Chronic disease, Sideroblastic.
| Master Comparison: Microcytic Anemias | ||||
|---|---|---|---|---|
| Feature | IDA | Thalassemia | Anemia of Chronic Disease | Sideroblastic Anemia |
| MCV | ↓ | ↓↓ (disproportionate to anemia) | Normal or mildly ↓ | ↓ (or dimorphic) |
| RDW | ↑↑ (high-yield differentiator) | Normal | Normal | ↑ |
| RBC count | ↓ | Normal or ↑ | ↓ | ↓ |
| Serum iron | ↓ | Normal | ↓ | ↑↑ |
| Ferritin | ↓↓ (most specific) | Normal or ↑ | ↑ (acute-phase reactant) | ↑↑ |
| TIBC | ↑ | Normal | ↓ | Normal or ↓ |
| Transferrin sat. | ↓ (<15%) | Normal or ↑ | Normal or ↓ | ↑↑ |
| Smear clue | Pencil cells, anisocytosis | Target cells, basophilic stippling | Nonspecific | Pappenheimer bodies |
| Gold standard | Iron studies | Hb electrophoresis | Identify underlying inflammation | Bone marrow (ringed sideroblasts) |
Key differentiation pearls:
- IDA vs Thalassemia: RDW is ↑ in IDA, normal in thalassemia. RBC count is ↓ in IDA, normal/↑ in thalassemia. Mentzer index (MCV/RBC): >13 → IDA; <13 → thalassemia.
- IDA vs ACD: ferritin ↓ in IDA, ↑ in ACD. TIBC ↑ in IDA, ↓ in ACD.
| ملاحظة سريرية – Clinical Note | |
| ارتفاع RDW هو علامة مميزة لنقص الحديد، بينما يكون طبيعياً في الثلاسيميا. كذلك عدد كريات الدم الحمراء (RBC count) منخفض في نقص الحديد ومرتفع أو طبيعي في الثلاسيميا. | ملاحظة |
See the Iron Studies in Microcytic Anemia: Comparison Table for a side-by-side reference of the iron-study patterns, and the Iron Deficiency Anemia vs Alpha-Thalassemia Minor vs Beta-Thalassemia Minor: Comparison Table for thalassemia-specific differentiators.
Step 4 — Find the cause (mandatory — never just "give iron")
- Adult men & postmenopausal women → upper endoscopy + colonoscopy (rule out GI malignancy until proven otherwise)
- Premenopausal women → detailed menstrual history; if menses normal → GI workup
- Children → dietary history (cow's milk excess, lack of iron-fortified foods); screen for celiac disease if no response to iron
- Suspected malabsorption → anti-tissue transglutaminase IgA (celiac), H. pylori testing
Management
Two parallel tasks: (1) replace iron and (2) treat the underlying cause. Never give iron without investigating the source.
1. Oral iron — first-line
- Ferrous sulfate 325 mg PO once daily or every other day (contains ~65 mg elemental iron per tablet).
- Every-other-day dosing improves fractional absorption by lowering the hepcidin response and reduces GI side effects.
- Alternatives: ferrous gluconate 325 mg PO (36 mg elemental iron) or ferrous fumarate 325 mg PO (106 mg elemental iron) — similar efficacy.
- Take on an empty stomach with vitamin C / orange juice (↑ absorption by maintaining Fe²⁺ form).
- Avoid co-administration with antacids, PPIs, calcium, tea, coffee, milk, or phytate-rich foods (↓ absorption).
- Side effects: nausea, epigastric pain, constipation, black stools (harmless — warn the patient).
- Duration: continue iron for 3–6 months after Hb normalizes to replenish ferritin stores.
| Important – فكرة سؤال | |
| Iron chelates tetracyclines and fluoroquinolones. Oral iron supplements form insoluble complexes with these antibiotics in the GI tract, dramatically ↓ their absorption. Always separate dosing by ≥2 hours. This interaction is a high-yield USMLE pharmacology pearl. | تذكر |
2. IV iron — when oral fails or is not possible
- Indications: oral intolerance, malabsorption (celiac, post-bariatric), CKD on EPO, severe ongoing blood loss, IBD, or need for rapid correction (e.g., late pregnancy).
- Preparations:
- Ferric carboxymaltose: 750 mg IV, repeat after ≥7 days (max 1500 mg per course) — preferred for rapid repletion
- Iron sucrose: 200 mg IV per session (often used in CKD/dialysis patients)
- Iron dextran: requires test dose (risk of anaphylaxis); allows full repletion in a single infusion
3. Blood transfusion
- Reserved for severe anemia with hemodynamic instability, active hemorrhage, or symptomatic anemia with Hb <7 g/dL (lower threshold in cardiac disease).
4. Treat the underlying cause
- Stop offending drugs (NSAIDs, aspirin)
- Treat H. pylori (eradication therapy)
- Resect colon cancer / manage GI lesion
- Control menorrhagia (OCPs, levonorgestrel IUD, surgical options)
- Celiac disease → gluten-free diet
- Hookworm → albendazole 400 mg PO × 1 dose
Refer to the Iron-Rich Foods by Category for patient dietary counseling on iron-rich food sources.
| Note – Monitoring Treatment Response | |
| Reticulocytosis peaks at 5–7 days (first sign of response). Hb rises ~1 g/dL every 2–3 weeks; normalizes by 6–8 weeks. If no response by 4 weeks: reconsider diagnosis (thalassemia? ACD?), check compliance, ongoing blood loss, or malabsorption. |
ملاحظة |
For pediatric-specific screening and treatment thresholds, see the Iron Deficiency Anemia in Young Children: Risk Factors, Diagnosis, and Treatment reference.
Complications
Complications
- High-output heart failure — in severe, prolonged anemia
- Pregnancy: ↑ risk of preterm birth, low birth weight, maternal mortality from peripartum hemorrhage. See the Anemias in Pregnancy: Comparative Features by Type for the full differential in pregnancy.
- Children: impaired cognitive and motor development; poor school performance — may be irreversible if prolonged
- Plummer–Vinson syndrome: chronic IDA + esophageal web + dysphagia → ↑ risk of esophageal squamous cell carcinoma
- Restless legs syndrome — IDA is a recognized secondary cause (treat when ferritin ≤75 µg/L). See the Restless Legs Syndrome: Clinical Features, Secondary Causes, and Treatment for management details.
- Worsening of pre-existing cardiac or pulmonary disease
Clinical Pearls – نقاط مهمة للامتحانات
Consolidated Mnemonics – جمل تذكرية
| Mnemonic – Signs of Iron Deficiency: "PICA KOI" | |
| Pica (ice, dirt, clay) Impaired growth/cognition (children) Cheilitis (angular) Atrophic glossitis Koilonychia (spoon nails) Onset of restless legs Iron studies: ↓ ferritin, ↓ Fe, ↑ TIBC |
جملة تذكرية |
| Mnemonic – Iron Studies in IDA: "Low-Low-High-Low" | |
| Low serum iron → Low ferritin → High TIBC → Low transferrin saturation The body is "hungry" for iron → builds more transport trucks (TIBC ↑) but the trucks are mostly empty (saturation ↓). |
جملة تذكرية |
Key Exam Pearls – نقاط مهمة للامتحانات
- Most common anemia worldwide and the most common cause of microcytic hypochromic anemia.
- Premenopausal women → think menstrual loss. Men & postmenopausal women → think GI bleed / colon cancer until proven otherwise.
- Ferritin is the most specific test — ↓ ferritin is diagnostic. Beware the acute-phase reactant trap (see Arabic note above).
- Classic iron-study pattern: ↓ Fe, ↓ ferritin, ↑ TIBC, ↓ transferrin saturation.
- ↑ RDW distinguishes IDA from thalassemia (normal RDW in thalassemia).
- Pica (especially pagophagia / ice craving) is a buzzword for IDA on exams.
- Early IDA may be normocytic. MCV falls late; iron studies are abnormal before MCV drops. A young woman with heavy menses and normocytic anemia still needs iron studies.
- First-line = oral ferrous sulfate on empty stomach with vitamin C. Expect reticulocytosis in ~1 week; Hb correction by 6–8 weeks; continue 3–6 months after Hb normalizes.
- Iron is absorbed in the duodenum as Fe²⁺; gastric acid is essential for conversion. Hepcidin is the master regulator — ↓ in IDA, ↑ in ACD (blocking ferroportin).
- Celiac disease may present with IDA as the only finding (no GI symptoms) — screen with anti-tTG IgA if IDA is refractory to oral iron or malabsorption is suspected.
- Never give iron without looking for the source.
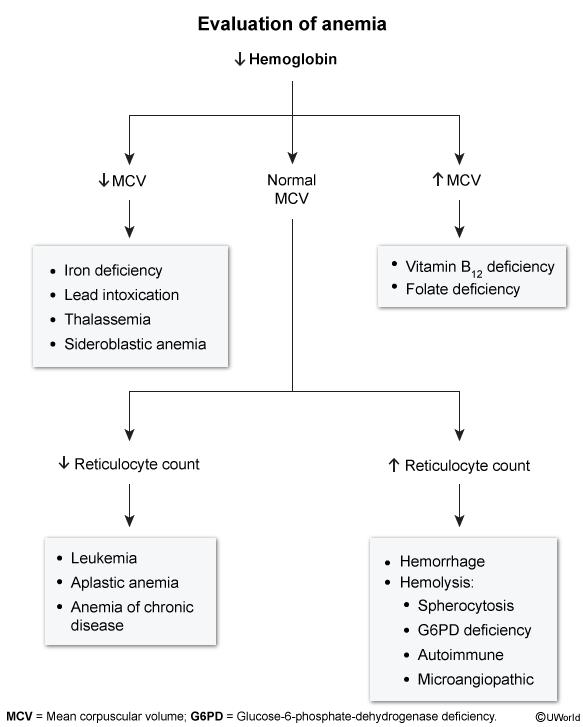
For the complete diagnostic algorithm for anemia evaluation by MCV and reticulocyte count, refer to the anemia evaluation flowchart presented in the Diagnostic Approach section above.
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.