سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Background
- Hydrocephalus is derived from the Greek word "hudro" which means water and “kephale” which means head
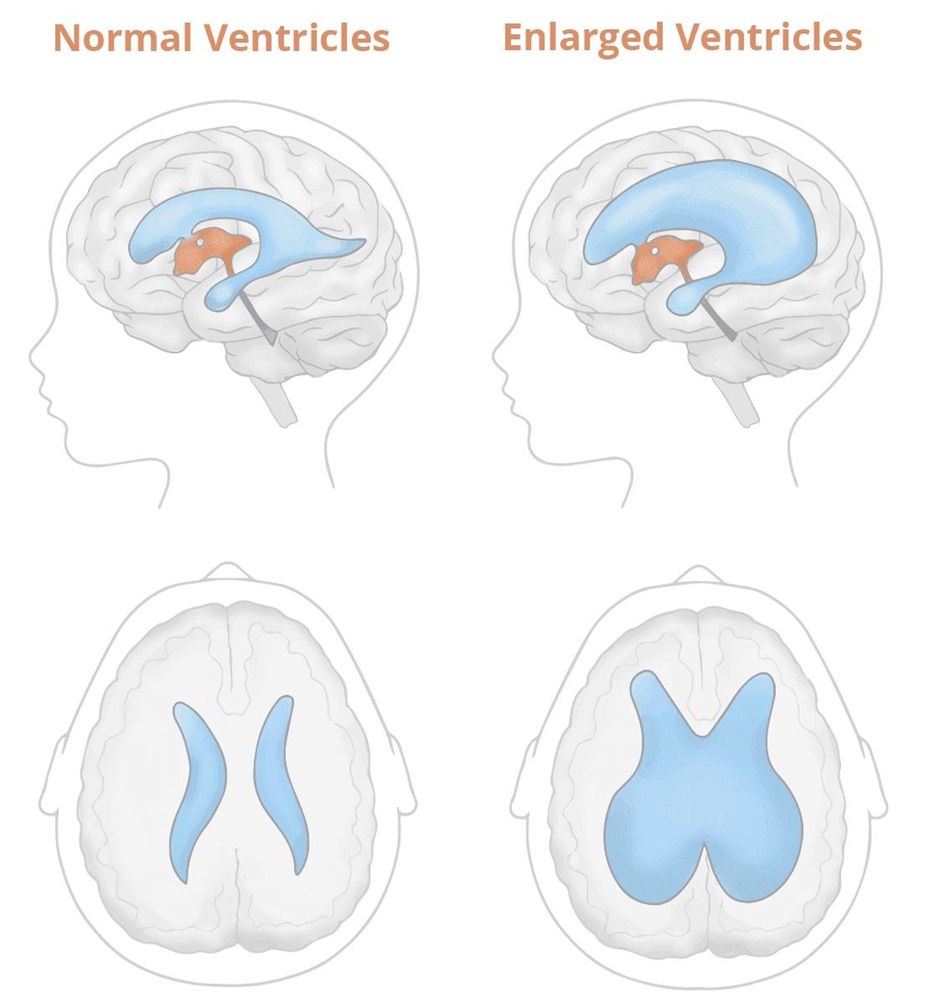
- Hydrocephalus: an abnormal enlargement of the ventricles due to an excessive accumulation of the cerebrospinal fluid resulting from a disturbance of its flow, absorption, or uncommonly, secretion
- This increase of CSF within the central nervous system results in increased intracranial pressure (ICP)
- Hydrocephalus ex vacuo: an enlargement of CSF due to brain atrophy without an actual increase in ICP
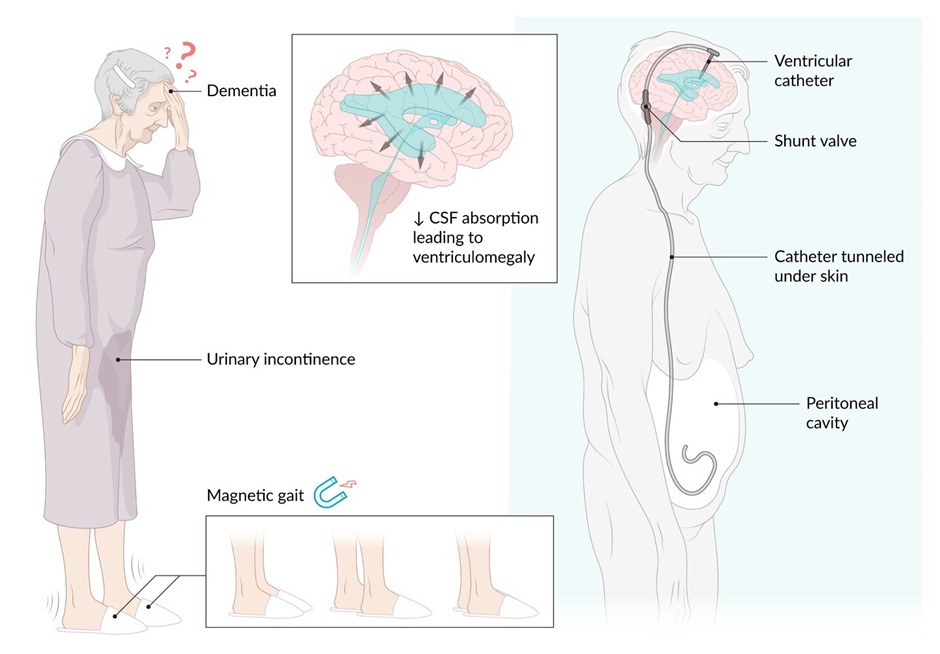
- Normal pressure hydrocephalus: a condition with enlarged ventricles but normal ICP
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Physiology
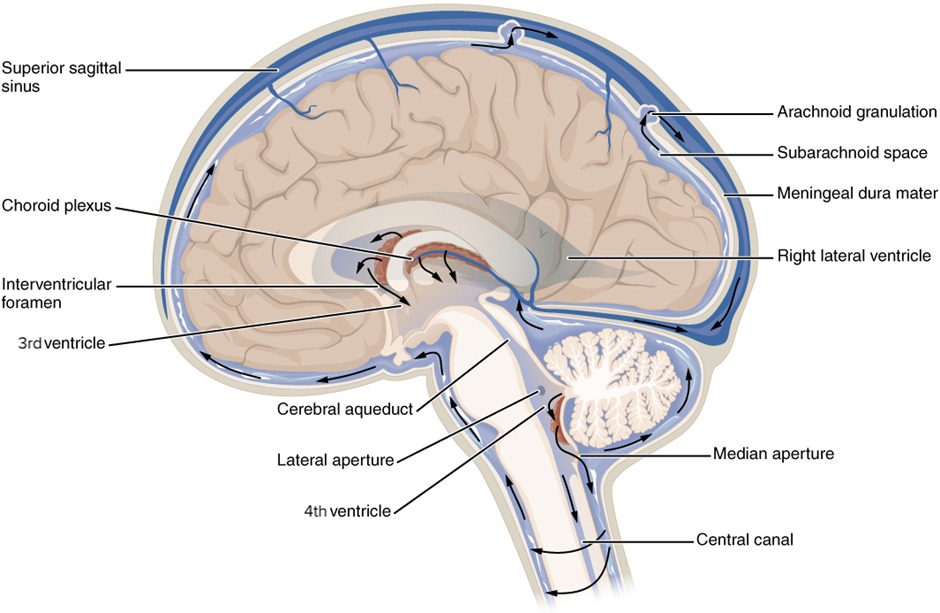
- Secretion of the CSF: choroid plexus in the ventricles
- CSF rate of production: 0.4 ml per minute (500 ml in 24 hours) the normal volume of CSF is 140 ml
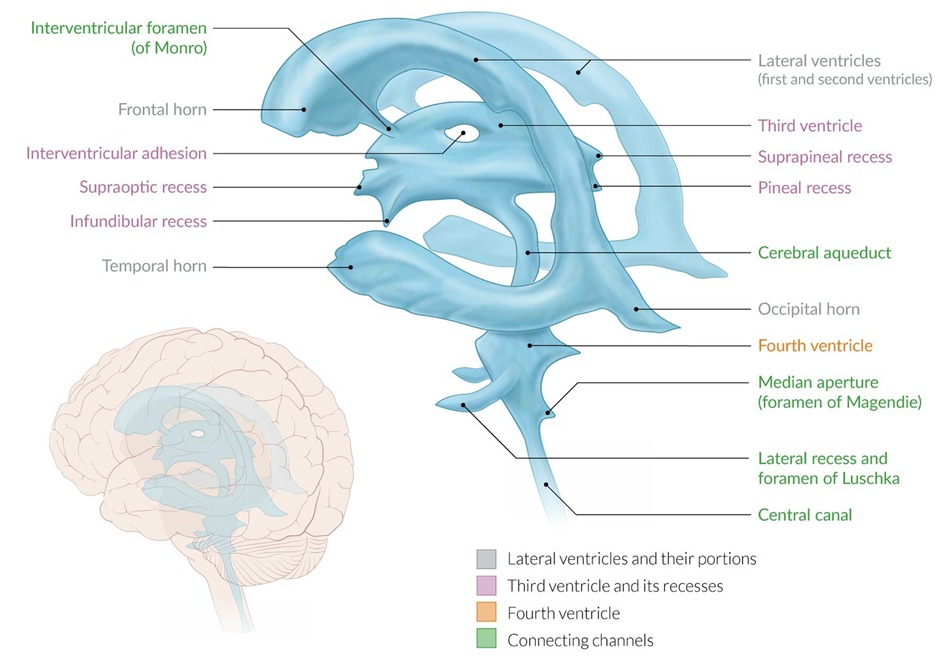
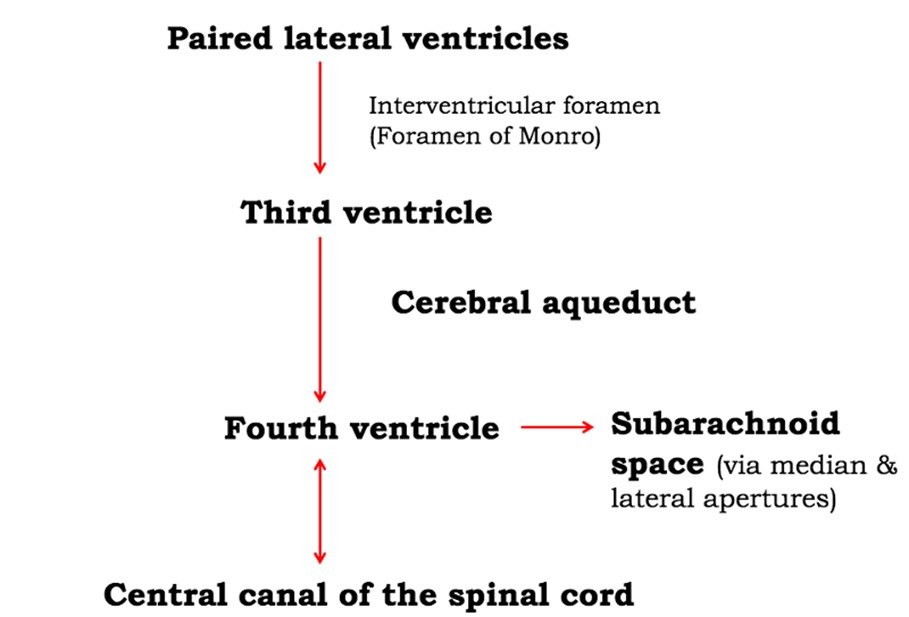
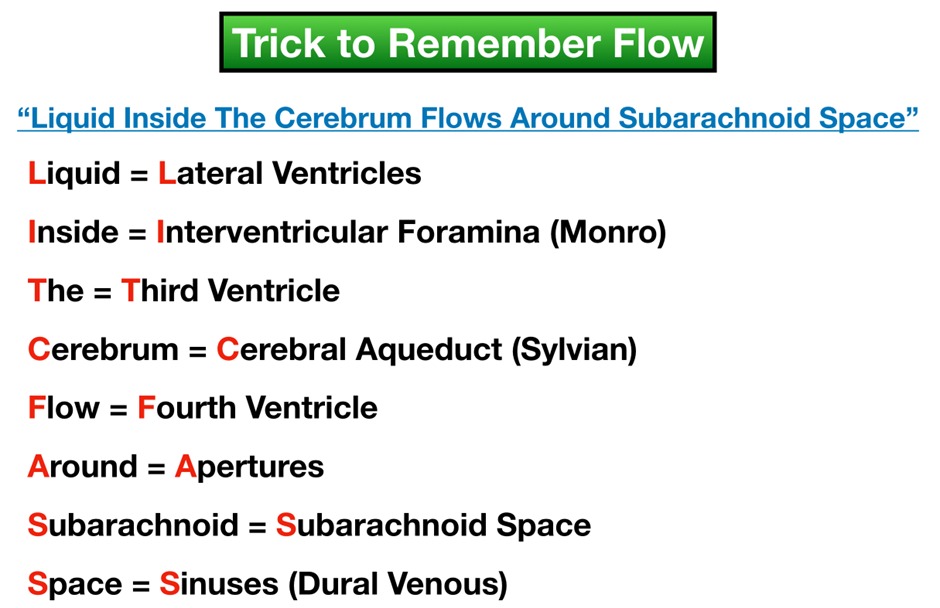
- Direction of flow: CSF flows from the lateral ventricles through the foramen of Monro into the third ventricle, via the aqueduct of Sylvius into the fourth ventricle and then through the foramina of Magendie (1 foramen) and Luschka (2 foramina) into the subarachnoid space and basal cisterns
- Absorption of the CSF: CSF is absorbed by the arachnoid villi of the dural sinuses
| Note | |
|
Luschka is LATERAL Magendie is MEDIAL |
ملاحظة |
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
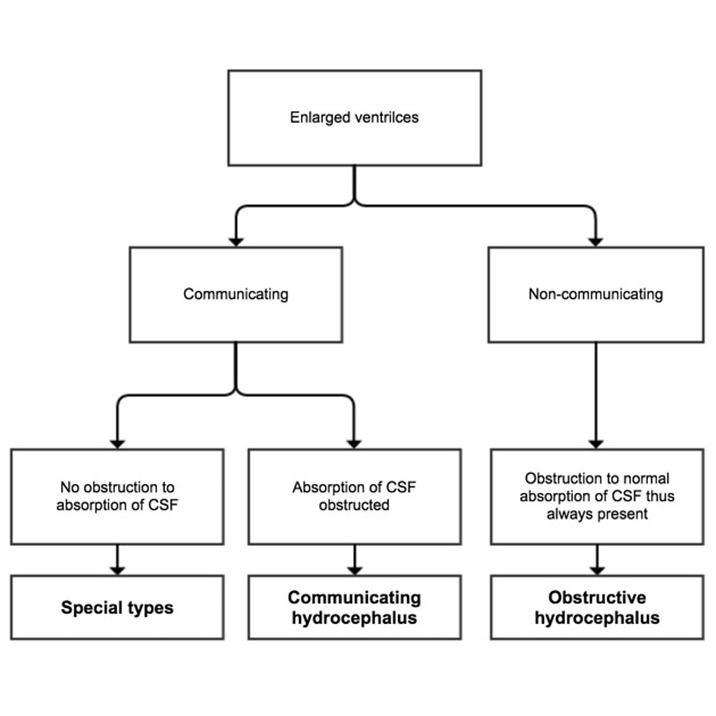
Classifications of Hydrocephalus
- Obstructive (noncommunicating) hydrocephalus (caused by obstruction to the flow of CSF within the ventricular system)
- Communicating hydrocephalus (there’s no obstruction to the flow of CSF flow within the ventricular system; usually failure of absorption of CSF by the arachnoid granulations)
| Obstructive hydrocephalus | Communicating hydrocephalus |
|---|---|
|
|
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Clinical Presentation
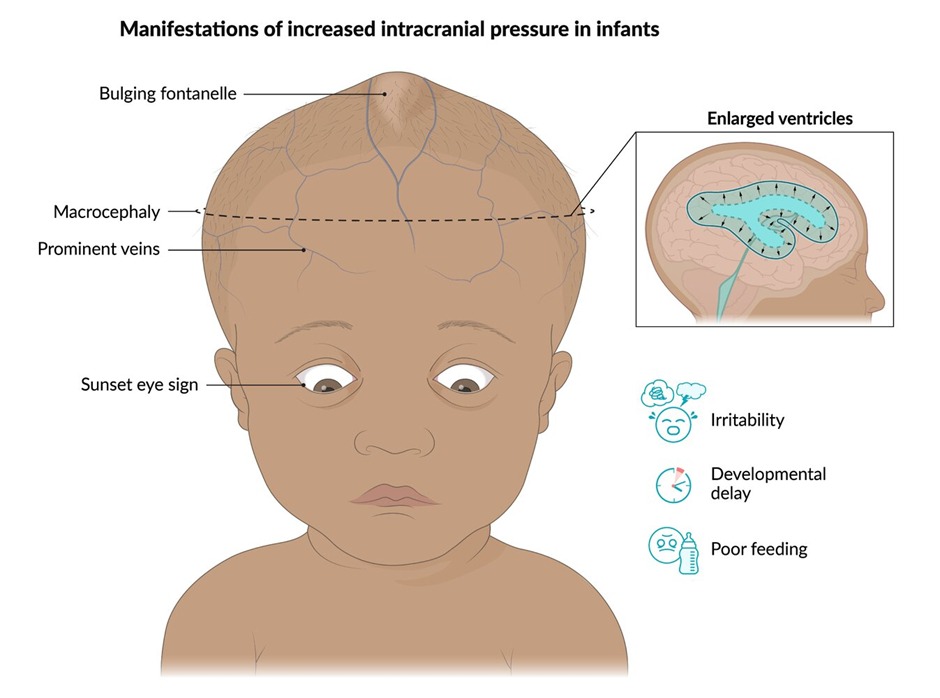
- Majority of children with hydrocephalus present at birth or shortly thereafter, but in paediatrics symptoms vary by age due to the presence of open cranial sutures
- After the cranial sutures and fontanelles are closed, the patients’ symptoms are more closely related to elevated ICP
- At birth when the cranial sutures are still open, infants more commonly present with increasing head circumference
- Prior to the fusion of cranial sutures, infants most commonly present subacutely with increasing head circumference. Children typically become irritable before progressing to vomiting or restricted upgaze
| infant | children |
|---|---|
|
|
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Diagnosis
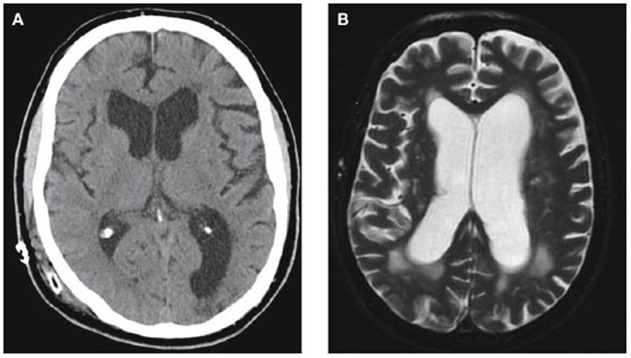
- The most important investigational imaging modalities are either a CT scan or MRI of the brain, which will show which ventricles are dilated. An enhanced CT scan or MRI will help determine the cause, as it will better define the presence of an obstructing tumor
- Ultrasound through open anterior Fontanelle is useful in assessing ventricular size in infants
- Plain skull X-ray may demonstrate splayed sutures
- Records of the head circumference and its comparisons with body, weight and length charts are an integral part of postnatal follow-up for any child
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Treatment
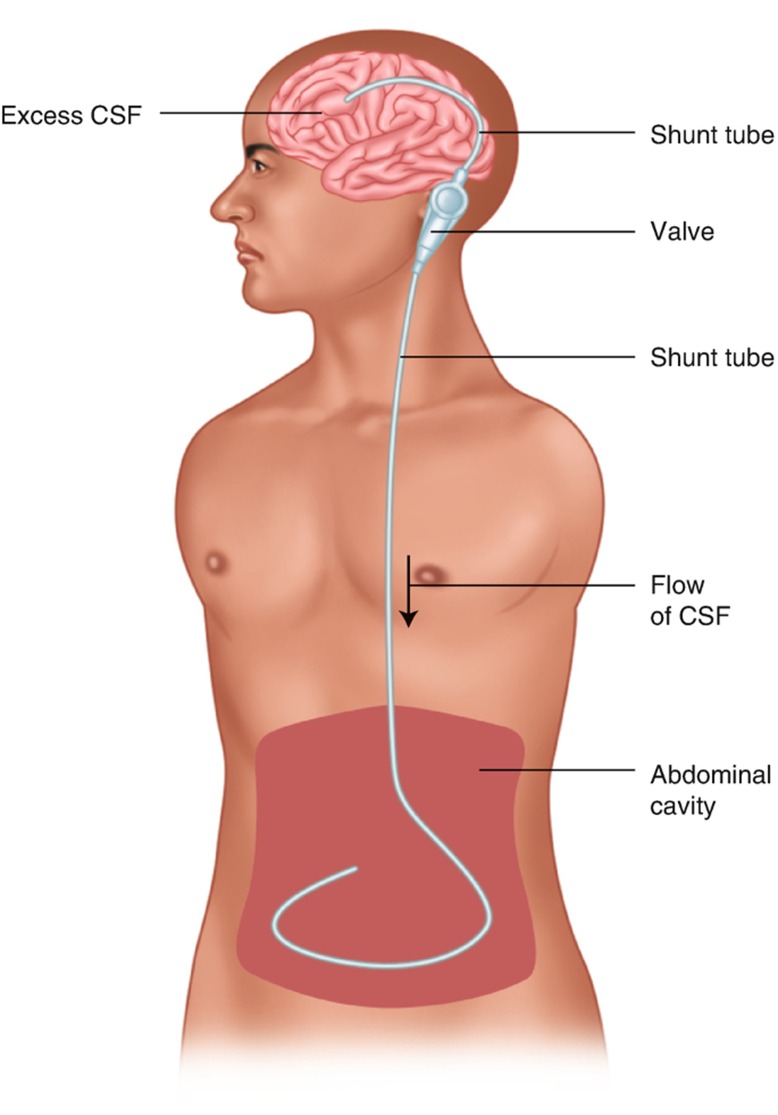
- Permanent surgical solutions to hydrocephalus include CSF shunting and endoscopic third ventriculostomy (ETV) with and without choroid plexus coagulation (CPC)
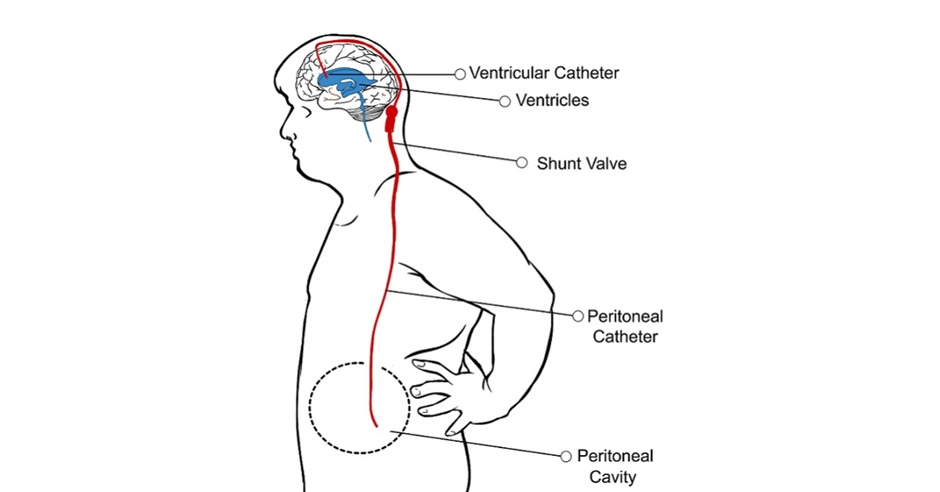
- A shunt is a permanent CSF diversion device with 3 components: a ventricular catheter, a valve, and a distal catheter (Programmable systems and non programmable systems)
- Despite advances in shunt hardware including antibiotic impregnated tubing, shunt infection remains an extraordinarily common morbid and costly complication
- The preferred method of shunting remains VP shunting, but other common distal locations include pleural and atrial
- Shunt blockage may occur up to 30% to 40% within the first year after shunt insertion. Infection occurs in about 8% of shunt procedures
- Although the continuation of the antibiotics for 24-36 hours postoperatively has not been proven to be effective, it is a reasonable precaution
- An infected shunt needs to be removed and replaced
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Supplemental materials
| Hydrocephalus in children | |
|---|---|
| Content |
|
| Clinical manifestations |
|
| Evaluation |
|
| Normal pressure hydrocephalus | |
|---|---|
| Clinical features |
|
| Diagnosis |
|
| Treatment |
|
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.
فيديوهات الشرح
بطاقات تفاعلية
أسئلة ممارسة
اشترك الآن