Summary
Inflammatory bowel disease (IBD) is a group of chronic, relapsing inflammatory disorders of the GI tract caused by an abnormal immune response to gut flora in genetically susceptible individuals.
- Two main subtypes: Crohn disease (CD) and ulcerative colitis (UC).
- Classic presentation: recurrent bloody diarrhea, abdominal pain, weight loss, and fever.
- Diagnosis is confirmed by endoscopy + biopsy.
- Treated with anti-inflammatory drugs (mesalamine, azathioprine, 6-MP, anti-TNF); flares treated with steroids.
- Surgery is curative in UC, but reserved for complications in CD.
Definition
- IBD = chronic, relapsing inflammation of the bowel due to an abnormal immune response to enteric flora.
- Subclassified into two main entities:
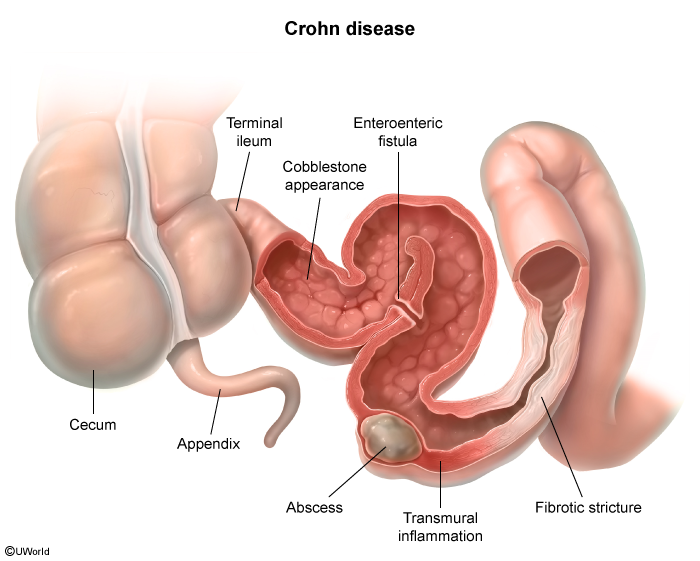
- Crohn disease (CD) – any part of the GI tract (mouth to anus); transmural inflammation.
- Ulcerative colitis (UC) – limited to colon/rectum; mucosal & submucosal only.
- Both are idiopathic, present with diarrhea, abdominal pain, weight loss, and bleeding.
Epidemiology
- Peak onset: adolescence and young adulthood.
- In pediatric IBD: ~4% present before age 5, ~18% before age 10.
- Sex differences:
- Girls → more likely to develop Crohn disease.
- Boys → more likely to develop ulcerative colitis.
- More common in Caucasians, especially Ashkenazi Jews.
Etiology and Risk Factors
The exact cause of IBD is unknown. It results from an interaction between genetics + environment + immune dysregulation in a susceptible host.
- Genetic susceptibility – NOD2/CARD15 mutations associated with CD; positive family history is the strongest risk factor.
- Environmental triggers:
- Smoking (↑ CD, ↓ UC).
- Hygiene hypothesis.
- Enteric microorganisms / altered microbiome.
- Diet, NSAIDs, stress.
- Immune response: abnormal T-cell activation against normal gut flora → chronic inflammation.
| Mnemonic – Smoking and IBD | |
Smoking is protective in UC but harmful in CD. Remember: "Smoking Causes Crohn" (S-C-C). |
جملة تذكرية |
Crohn Disease vs Ulcerative Colitis
The two IBD subtypes share many features but differ in location, depth, and complications. Compare them side-by-side using the IBD subtype characteristics reference table.
| Crohn Disease vs Ulcerative Colitis | ||
|---|---|---|
| Feature | Crohn Disease (CD) | Ulcerative Colitis (UC) |
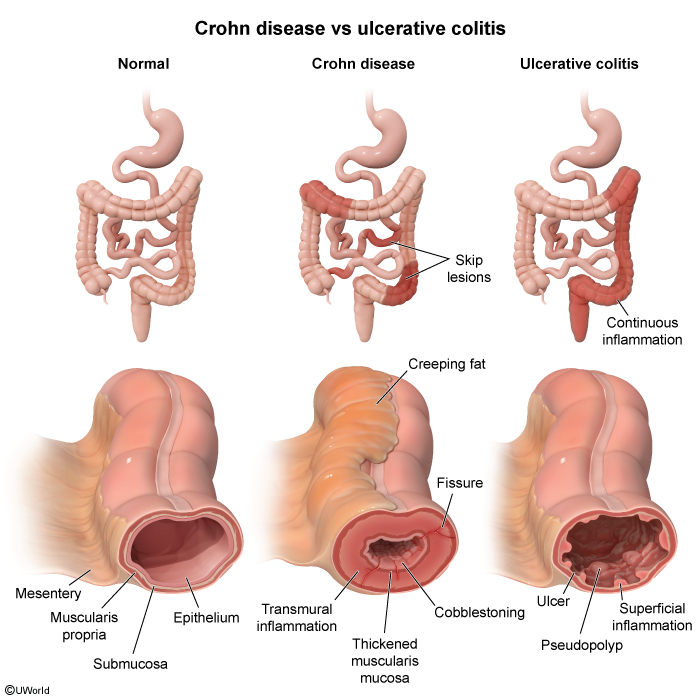
| Location | Mouth → anus (mostly terminal ileum + colon); rectal sparing; skip lesions | Rectum (always) ± colon; continuous involvement |
| Depth of inflammation | Transmural (entire bowel wall) | Mucosa + submucosa only |
| Microscopy | Noncaseating granulomas | Crypt abscesses, no granulomas |
| Gross findings | Cobblestoning, creeping fat, linear ulcers, strictures, fistulas | Pseudopolyps, friable erythematous mucosa, loss of haustra ("lead-pipe" colon) |
| Diarrhea | Watery (bloody only if colon involved) | Bloody diarrhea (always) |
| Abdominal pain | Often RLQ (ileal disease) | LLQ / crampy |
| Complications | Fistulae, abscesses, strictures, obstruction, malabsorption, gallstones, kidney stones | Toxic megacolon, primary sclerosing cholangitis, colorectal cancer |
| Smoking effect | Worsens disease | Protective |
| Surgery | Not curative (reserved for complications) | Curative (total colectomy) |
Pathology
The hallmark histological and gross findings are the highest-yield distinguishing features.
Crohn Disease
- Transmural inflammation with noncaseating granulomas (pathognomonic).
- Knife-like fissuring ulcers extending through all bowel layers.
- Cobblestoning, creeping fat, serpiginous ulcers on gross specimen.
- Skip lesions — areas of normal mucosa between diseased segments.
Ulcerative Colitis
- Mucosal + submucosal inflammation only (does not penetrate deeper layers).
- Crypt abscesses (neutrophils within crypts) — characteristic finding.
- Pseudopolyps, friable mucosa, loss of haustra ("lead-pipe colon").
- Inflammation is continuous starting at the rectum and extending proximally.
| Important – فكرة سؤال | |
|
تذكر |
Clinical Features
Shared Symptoms
- Chronic diarrhea, crampy abdominal pain.
- Weight loss, low-grade fever, fatigue.
- GI bleeding (more typical of UC).
Crohn Disease
- Insidious onset of abdominal pain (often RLQ), non-bloody diarrhea, weight loss.
- Palpable RLQ mass (transmural inflammation of terminal ileum).
- Perianal disease: skin tags, fissures, fistulas, abscesses.
- Oral ulcers (aphthous), malabsorption (B12, fat → steatorrhea).
Ulcerative Colitis
- Bloody diarrhea with mucus and tenesmus.
- LLQ pain, urgency, low-grade fever.
- No perianal/oral disease and no fistulas.
Extraintestinal Manifestations (both CD & UC)
- Eye: episcleritis, scleritis, uveitis.
- Skin: erythema nodosum, pyoderma gangrenosum.
- Joints: peripheral arthritis, ankylosing spondylitis, sacroiliitis.
- Liver: primary sclerosing cholangitis (PSC) — strongly linked to UC.
- Renal: calcium oxalate stones (enteric hyperoxaluria) — typical of CD.
- Biliary: cholesterol gallstones in CD (bile acid malabsorption).
Diagnosis
Initial Workup
- Labs: leukocytosis, iron-deficiency anemia, ↑ ESR/CRP, ↓ albumin.
- Stool studies: fecal calprotectin/lactoferrin (↑); exclude infection (C. difficile, ova/parasites).
- Antibodies (supportive, not diagnostic):
- p-ANCA → ulcerative colitis.
- ASCA (anti-Saccharomyces cerevisiae) → Crohn disease.
Confirmatory Test
- Endoscopy + biopsy is the gold standard.
- Colonoscopy with ileoscopy for suspected CD.
- Flexible sigmoidoscopy/colonoscopy for UC.
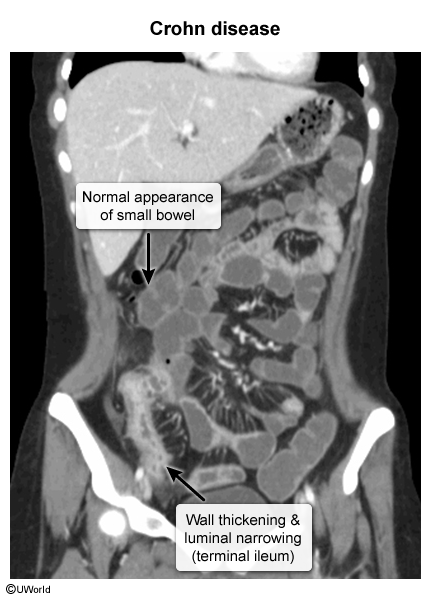
Imaging
- CT/MR enterography in CD: terminal ileum wall thickening, "string sign" (luminal narrowing), strictures, fistulas, abscesses.
- Avoid colonoscopy in acute severe colitis (risk of perforation/toxic megacolon) — use abdominal X-ray.
| Why Crohn causes kidney + gallstones | |
Terminal ileum disease in CD → bile acid malabsorption:
|
ملاحظة |
Differential Diagnosis
- Infectious gastroenteritis – acute, self-limited; stool cultures positive (Salmonella, Shigella, Campylobacter, Yersinia, E. coli O157:H7).
- C. difficile colitis – recent antibiotic use; toxin assay positive.
- Celiac disease (sprue) – chronic diarrhea, weight loss; anti-tTG IgG/IgA positive; duodenal biopsy shows villous atrophy.
- Diverticulitis – older patient, LLQ pain, fever; CT shows inflamed diverticula.
- Irritable bowel syndrome (IBS) – no weight loss, no bleeding, normal labs and endoscopy.
- Intestinal TB – mimics Crohn (ileocecal involvement); biopsy shows caseating granulomas.
- Ischemic colitis – elderly patient, "watershed" areas (splenic flexure), bloody diarrhea.
Treatment
The goals of therapy are to induce remission during a flare and then maintain remission long-term. Choice of agent depends on disease severity, location, and subtype (UC vs. CD).
Medical therapy
- Mesalamine (5-ASA) derivatives are the standard therapy — first-line for mild–moderate disease, especially ulcerative colitis. Includes mesalamine and sulfasalazine; given orally for extensive disease or as suppository/enema for distal UC.
- Acute exacerbations are treated with high-dose corticosteroids — oral prednisone for moderate flares, IV hydrocortisone or methylprednisolone for severe flares. Budesonide is preferred for ileal Crohn's (first-pass hepatic metabolism → fewer systemic effects). Never used for maintenance.
- Immunomodulators (azathioprine, 6-mercaptopurine, methotrexate) — steroid-sparing maintenance agents. Check TPMT activity before starting azathioprine to avoid life-threatening myelosuppression.
- Biologics for moderate–severe or refractory disease — anti-TNF (infliximab, adalimumab), anti-integrin (vedolizumab), anti-IL-12/23 (ustekinumab).
- Antibiotics (metronidazole, ciprofloxacin) — useful for perianal Crohn's and fistulizing disease.
Surgical therapy
- Surgery is curative in ulcerative colitis — total proctocolectomy removes the diseased organ entirely. Indicated for refractory disease, dysplasia/cancer, or toxic megacolon.
- Surgery in Crohn's disease is reserved for complications — fistulae, strictures, abscesses, obstruction, or perforation. Limited bowel-sparing resection only; disease inevitably recurs at the anastomosis, so surgery is not curative.
| High-Yield Treatment Pearls | |
|
تذكر |
Complications
IBD complications fall into three buckets — those shared between Crohn and UC, those that are Crohn-specific (driven by transmural inflammation and terminal-ileum disease), and those that are UC-specific (driven by mucosal, continuous colonic inflammation).
Shared (CD and UC)
- Colorectal cancer — risk rises after ~8–10 years of colonic involvement. Risk factors: longer duration, greater extent of colitis, PSC, family history. Surveillance colonoscopy every 1–2 years with random biopsies; use the IBD colonoscopy surveillance guidelines.
- GI bleeding and anemia (iron deficiency from chronic blood loss; B12 deficiency in Crohn with ileal disease).
- Malnutrition and weight loss (especially in Crohn with extensive small-bowel disease).
- Bowel perforation (more common with severe colitis or toxic megacolon).
- Venous thromboembolism (VTE) — IBD is a hypercoagulable state during flares (DVT/PE risk ↑).
Crohn-specific complications
Driven by transmural inflammation that tunnels through all layers of the bowel wall, plus terminal ileum dysfunction.
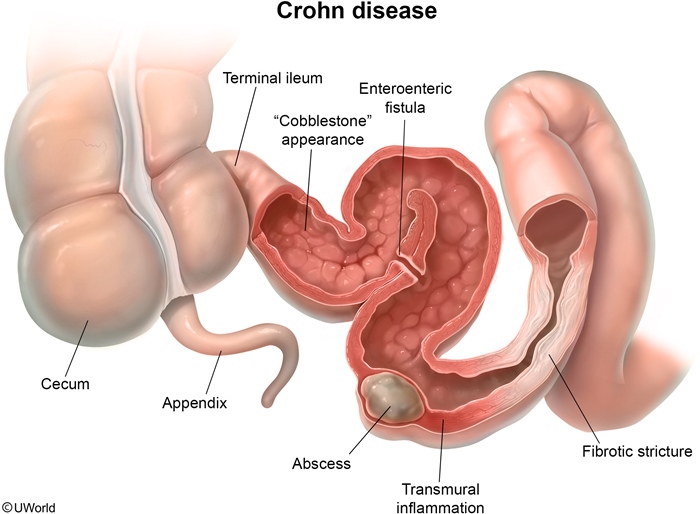
- Fistulas — abnormal tracts between bowel and adjacent structures from transmural inflammation:
- Enterocutaneous (bowel contents draining to skin)
- Enteroenteric (bowel-to-bowel)
- Enterovesical (recurrent UTIs, pneumaturia, fecaluria)
- Rectovaginal (stool from vagina)
- Perianal — see the perianal/anorectal fistula reference.
- Strictures → small bowel obstruction (SBO): crampy abdominal pain, vomiting, obstipation, dilated loops with air–fluid levels.
Link to the full SBO reference table for workup and management.
- Abscesses — intra-abdominal or perianal pus collections; drain + antibiotics + treat underlying disease.
- Terminal ileum disease/resection consequences:
- Cholesterol gallstones (↓ bile acid pool → cholesterol-supersaturated bile).
- Calcium-oxalate kidney stones (fat malabsorption → calcium binds fat → free oxalate absorbed → hyperoxaluria).
- Vitamin B12 deficiency (terminal ileum is the only B12 absorption site) → macrocytic anemia, neuropathy.
- Fat-soluble vitamin deficiencies (A, D, E, K) from bile-acid loss and steatorrhea.
- Perianal disease — skin tags, fissures, fistulas, abscesses. Very characteristic of Crohn.
| Mnemonic — Crohn intestinal complications: FSA | |
Fistulas — transmural inflammation tunnels through the wall (enterocutaneous, enteroenteric, enterovesical, rectovaginal, perianal). Strictures — fibrosis narrows the lumen → small-bowel obstruction. Abscesses — walled-off pus collections from perforating disease. Think "FSA = the three intestinal complications Crohn loves to test." |
جملة تذكرية |
| Mnemonic — Stones in Crohn: "Terminal ileum → 2 kinds of stones" | |
Terminal ileum disease/resection → loss of bile-acid reabsorption →
Plus B12 deficiency — terminal ileum is the only site of B12 absorption. |
جملة تذكرية |
UC-specific complications
Driven by continuous mucosal inflammation of the colon.
- Toxic megacolon — surgical emergency; severe colitis paralyzes the colonic smooth muscle.
Full workup/management in the toxic megacolon reference table.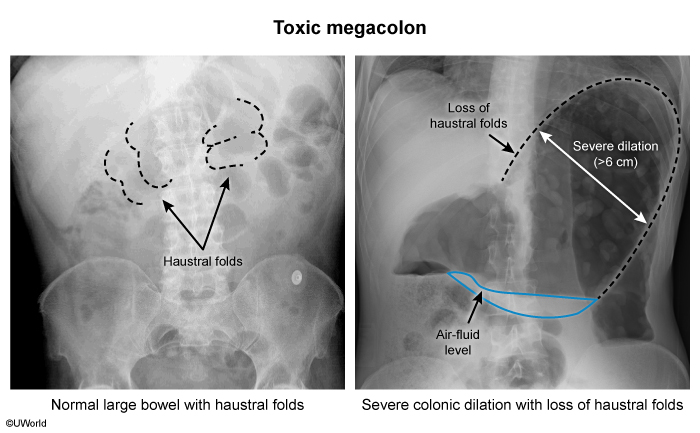
- Primary sclerosing cholangitis (PSC) — chronic inflammation/fibrosis of intra- and extra-hepatic bile ducts.
- MRCP: "beaded" bile ducts (alternating strictures and dilations).
- Labs: ↑ alkaline phosphatase; p-ANCA positive.
- Complications: recurrent cholangitis, cholangiocarcinoma, and a further ↑ in colorectal cancer risk. Open the PSC reference table for full features.
- Higher cumulative colorectal cancer risk than CD (entire colon continuously inflamed).
- Severe hemorrhage from diffuse mucosal ulceration.
- Perforation — usually in the context of toxic megacolon or severe fulminant colitis.
| Complications at a glance: Crohn vs Ulcerative colitis | ||
|---|---|---|
| Complication | Crohn disease | Ulcerative colitis |
| Fistulas | ✅ Common (transmural) | ❌ Rare |
| Strictures / obstruction | ✅ Common | Rare |
| Abscesses | ✅ Common | Rare |
| Toxic megacolon | Uncommon | ✅ Classic (most feared) |
| Perforation | Possible | ✅ (severe colitis / toxic megacolon) |
| Colorectal cancer | ↑ (colonic involvement) | ✅✅ Higher cumulative risk |
| Primary sclerosing cholangitis | Rare | ✅ Classic association |
| Gallstones / kidney stones | ✅ (terminal ileum) | ❌ |
| B12 deficiency | ✅ (terminal ileum) | ❌ |
| Important – Question Idea | |
Toxic megacolon = life-threatening complication, most classic in UC (also severe colitis from C. difficile).
|
تذكر |
Mnemonics
| Mnemonics – IBD high-yield | |
Crohn = "CHRISTMAS"
UC = "ULCCCERS"
Extraintestinal manifestations = "A PIE SAC": Arthritis, Pyoderma gangrenosum, Iritis/uveitis, Erythema nodosum, Sclerosing cholangitis, Aphthous ulcers, Clubbing. |
جملة تذكرية |
Key Points for Exams
- Crohn ≠ Ulcerative colitis: transmural + skip + granuloma vs. continuous + mucosal + crypt abscess.
- Bloody diarrhea → think UC first.
- RLQ pain + perianal disease + fistula → think Crohn.
- p-ANCA = UC; ASCA = Crohn.
- Smoking: protects UC, worsens Crohn.
- Endoscopy + biopsy = gold standard diagnosis.
- Steroids for flares, never for maintenance.
- Anti-TNF (infliximab, adalimumab): screen for TB + HBV first.
- Total colectomy curative in UC; surgery in CD is for complications only.
- Colon cancer surveillance begins 8–10 years after diagnosis (colonic involvement).
- PSC + UC association is a classic exam pearl.
- Toxic megacolon = no colonoscopy; consider urgent colectomy.
| نقاط مهمة للامتحان | |
|
ملاحظة |
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.