Summary
Von Willebrand Disease (vWD) is the most common inherited bleeding disorder, caused by a quantitative or qualitative defect in von Willebrand factor (vWF).
- Inheritance: Autosomal dominant (most types).
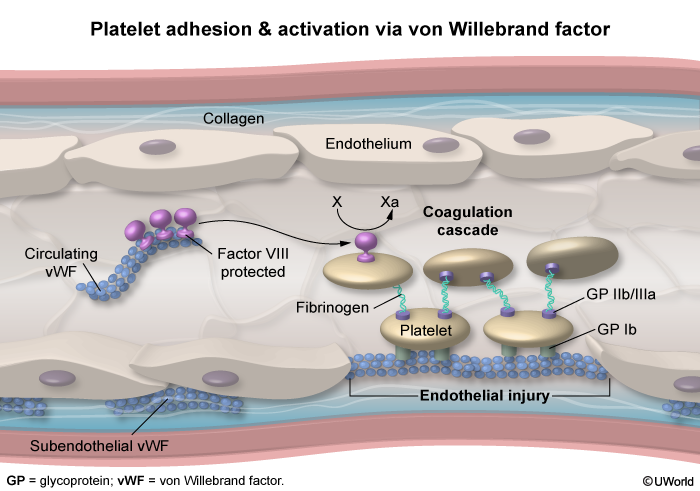
- vWF roles: (1) binds platelets to subendothelial collagen, (2) carries and protects Factor VIII.
- Bleeding pattern: Mucocutaneous → epistaxis, gum bleeding, menorrhagia, easy bruising.
- Classic labs: Normal platelet count, ↑ bleeding time / ↑ PFA-100, ↑ aPTT (due to ↓ Factor VIII), normal PT.
- Confirmatory test: ↓ Ristocetin cofactor activity.
- Treatment: Desmopressin (DDAVP) for type 1; vWF concentrate for severe types.
Definition and Epidemiology
Von Willebrand Disease is a bleeding disorder due to a deficiency or dysfunction of von Willebrand factor (vWF), a glycoprotein synthesized by endothelial cells and megakaryocytes and stored in Weibel-Palade bodies (endothelium) and platelet α-granules.
Key facts
- Most common inherited bleeding disorder (prevalence ~1%).
- Inheritance: Autosomal dominant in types 1 and 2; autosomal recessive in type 3.
- Sex distribution: Affects males and females equally — but women present more often (menorrhagia, postpartum bleeding).
- Onset: Usually mild; often diagnosed in adolescence/adulthood after surgery, dental work, or heavy menses.
Pathophysiology
What vWF does
- Platelet adhesion (primary hemostasis): At a site of vascular injury, vWF binds exposed subendothelial collagen and then binds platelet GPIb receptor → anchors platelets to the vessel wall.
- Factor VIII carrier: vWF circulates bound to Factor VIII, protecting it from proteolysis. Without vWF, FVIII half-life drops sharply → functional FVIII deficiency.
Consequences of vWF defect
- Impaired platelet plug → mucocutaneous bleeding (skin, mucous membranes).
- Low Factor VIII → mildly prolonged aPTT (intrinsic pathway).
- Platelet number is normal — only platelet function is impaired.
| Mnemonic – Functions of vWF | |
"vWF = velcro + FVIII carrier"
Lose vWF → you lose both primary hemostasis (platelet plug) and intrinsic pathway support (↓ FVIII → ↑ aPTT). |
جملة تذكرية |
Think of primary hemostasis as three steps — vWD blocks step 1 (adhesion), while Bernard-Soulier also blocks step 1 (GPIb defect) and Glanzmann blocks step 3 (GPIIb/IIIa defect).
Classification (Types of vWD)
Three main types — distinguished by whether vWF is reduced in quantity or defective in quality.
| Classification of Von Willebrand Disease: By mechanism of vWF defect | |
| Type 1 | Partial quantitative deficiency (most common, ~75%) |
| Inheritance | Autosomal dominant |
| vWF level | Mildly to moderately ↓ (functionally normal vWF) |
| Severity | Mild bleeding; responds well to DDAVP |
| Type 2 | Qualitative defect (~20%) — vWF is abnormal |
| 2A | Loss of high-molecular-weight multimers → ↓ platelet adhesion |
| 2B | Gain-of-function → vWF binds platelets spontaneously → thrombocytopenia. DDAVP is contraindicated |
| 2M | ↓ platelet binding without multimer loss |
| 2N | ↓ Factor VIII binding → mimics mild hemophilia A |
| Type 3 | Complete quantitative deficiency (rare, severe) |
| Inheritance | Autosomal recessive |
| vWF level | Virtually absent → very low FVIII |
| Presentation | Severe bleeding similar to hemophilia (hemarthrosis possible) |
Clinical Features
The bleeding pattern is mucocutaneous — typical of platelet-type bleeding — not deep tissue bleeding.
Common presentations
- Epistaxis (recurrent nosebleeds) — often the earliest sign in children.
- Gum bleeding, especially after brushing or dental procedures.
- Easy bruising and prolonged bleeding from small cuts.
- Menorrhagia — heavy menstrual bleeding is the most common presentation in women.
- Postpartum hemorrhage.
- GI bleeding — in older patients, may be associated with angiodysplasia.
- Excessive bleeding after surgery, tonsillectomy, or tooth extraction.
What you do NOT typically see
- Hemarthrosis or deep muscle hematoma → these suggest hemophilia, not vWD (exception: severe type 3 vWD).
- Petechiae are uncommon (platelet count is normal).
| Important – فكرة سؤال | |
Classic exam stem: young woman with heavy menstrual periods, easy bruising, and prolonged bleeding after dental extraction; family history of similar bleeding; normal platelet count, prolonged aPTT that corrects on mixing study. → Think Von Willebrand Disease. |
تذكر |
Diagnosis
Initial labs
- CBC: Normal platelet count (low only in type 2B).
- PT: Normal.
- aPTT: Normal or mildly prolonged (because of low FVIII). Corrects on mixing study — confirms a factor deficiency, not an inhibitor.
- Bleeding time / PFA-100 closure time: Prolonged → reflects defective platelet adhesion.
Confirmatory testing (vWD panel)
- vWF antigen (vWF:Ag) → quantitative level of vWF (low in types 1 and 3).
- Ristocetin cofactor activity (vWF:RCo) → best functional test; ristocetin induces vWF-mediated platelet agglutination. Low in all symptomatic types.
- Factor VIII activity → low (most marked in types 2N and 3).
- vWF multimer analysis → used to subclassify type 2.
- Ristocetin-induced platelet aggregation (RIPA): Increased in type 2B (platelets agglutinate even at low ristocetin doses).
The mixing study is a key step: the prolonged aPTT in vWD corrects because it reflects a factor deficiency (low FVIII), not an inhibitor.
Differential Diagnosis
Compare vWD with the two most common mimics on the exam — hemophilia A (deep bleeding, X-linked, normal platelets) and ITP (low platelets, mucocutaneous bleeding).
| vWD vs Hemophilia A vs ITP – High-yield differential | |||
|---|---|---|---|
| Feature | Von Willebrand Disease | Hemophilia A | ITP |
| Inheritance | Autosomal dominant (most) | X-linked recessive | Acquired (autoimmune) |
| Bleeding type | Mucocutaneous | Deep (hemarthrosis, muscle) | Mucocutaneous + petechiae |
| Platelet count | Normal | Normal | Low |
| Bleeding time / PFA | Prolonged | Normal | Prolonged |
| PT | Normal | Normal | Normal |
| aPTT | Normal or ↑ | ↑ (significantly) | Normal |
| Factor VIII | Normal or ↓ | ↓↓ | Normal |
| Treatment | DDAVP, vWF concentrate | Recombinant FVIII | Steroids, IVIG |
Other conditions to consider
- Hemophilia A and B — deep bleeding, hemarthrosis, prolonged aPTT, low FVIII or FIX.
- ITP — isolated low platelets, normal coagulation.
- Bernard-Soulier syndrome: GPIb receptor defect → cannot bind vWF; giant platelets, mild thrombocytopenia.
- Glanzmann thrombasthenia: GPIIb/IIIa defect → impaired platelet aggregation.
- Uremic platelet dysfunction: Acquired, in CKD; also responds to DDAVP.
Management
General principles
- Avoid antiplatelet drugs — no aspirin or NSAIDs.
- Treat minor bleeding with local measures (pressure, packing, tranexamic acid).
- Plan ahead for surgery and dental procedures with prophylactic treatment.
Specific therapies
- Desmopressin (DDAVP): First-line for type 1 (and mild type 2A). Releases stored vWF and FVIII from endothelium. Given IV or intranasally.
- vWF-containing concentrates (e.g., Humate-P, plasma-derived or recombinant vWF/FVIII concentrate): Used for types 2 and 3, major surgery, or severe bleeding.
- Antifibrinolytics: Tranexamic acid or aminocaproic acid — helpful for menorrhagia, dental, and mucosal bleeding.
- Combined oral contraceptives: Reduce menorrhagia by stabilizing the endometrium and slightly raising vWF/FVIII.
- Cryoprecipitate: Contains vWF, FVIII, fibrinogen — used only when concentrates are unavailable.
| Note – ملاحظة | |
DDAVP (desmopressin) is a synthetic ADH analog. In bleeding disorders, it stimulates release of pre-formed vWF and Factor VIII from Weibel-Palade bodies of endothelial cells.
|
ملاحظة |
For surgical patients, see the perioperative vWD management protocol and bleeding-risk stratification by procedure.
Complications
- Iron deficiency anemia from chronic mucosal blood loss (menorrhagia, GI bleeding).
- Postpartum hemorrhage — vWF rises during pregnancy but falls rapidly after delivery.
- Excessive surgical / dental bleeding if undiagnosed before procedure.
- GI bleeding from angiodysplasia — particularly in older patients with type 2A.
- Acquired vWD: A rare secondary form — seen with aortic stenosis (Heyde syndrome: aortic stenosis + GI angiodysplasia bleeding due to shear-induced destruction of large vWF multimers), lymphoproliferative disorders, hypothyroidism, and left ventricular assist devices.
Mnemonics
| Mnemonic – vWD essentials | |
"vWD = 1-2-3 + DDAVP"
"Bleeding pattern = Mucocutaneous" → think MEN: Menorrhagia, Epistaxis, Nosebleed/gum bleeding. |
جملة تذكرية |
Key Points for Exams
| Key Points for Exams – نقاط مهمة للامتحانات | |
|
تذكر |
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.