Summary
- PNH = acquired stem-cell disorder causing intravascular hemolysis, thrombosis, and bone marrow failure.
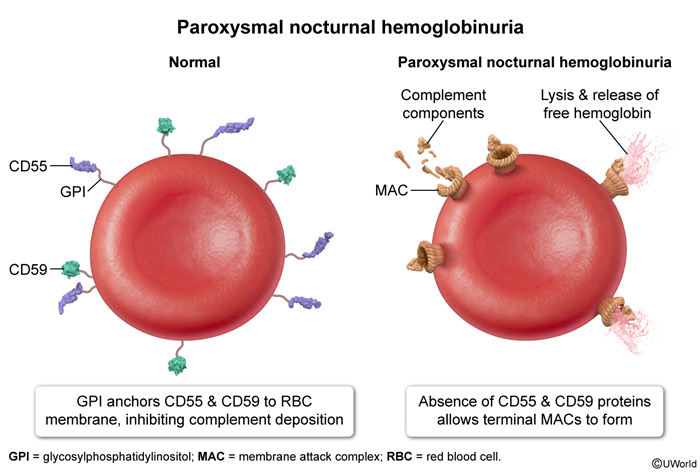
- Caused by an acquired somatic mutation in the PIGA gene → no GPI anchor → loss of CD55 and CD59 on blood cells.
- Without CD55/CD59, complement attacks RBCs → chronic intravascular hemolysis with episodic dark (cola-colored) morning urine.
- Classic triad: Coombs-negative hemolytic anemia + pancytopenia + venous thrombosis at unusual sites (hepatic, portal, cerebral veins).
- Diagnosis: flow cytometry showing absent CD55/CD59 (and FLAER negativity) on blood cells.
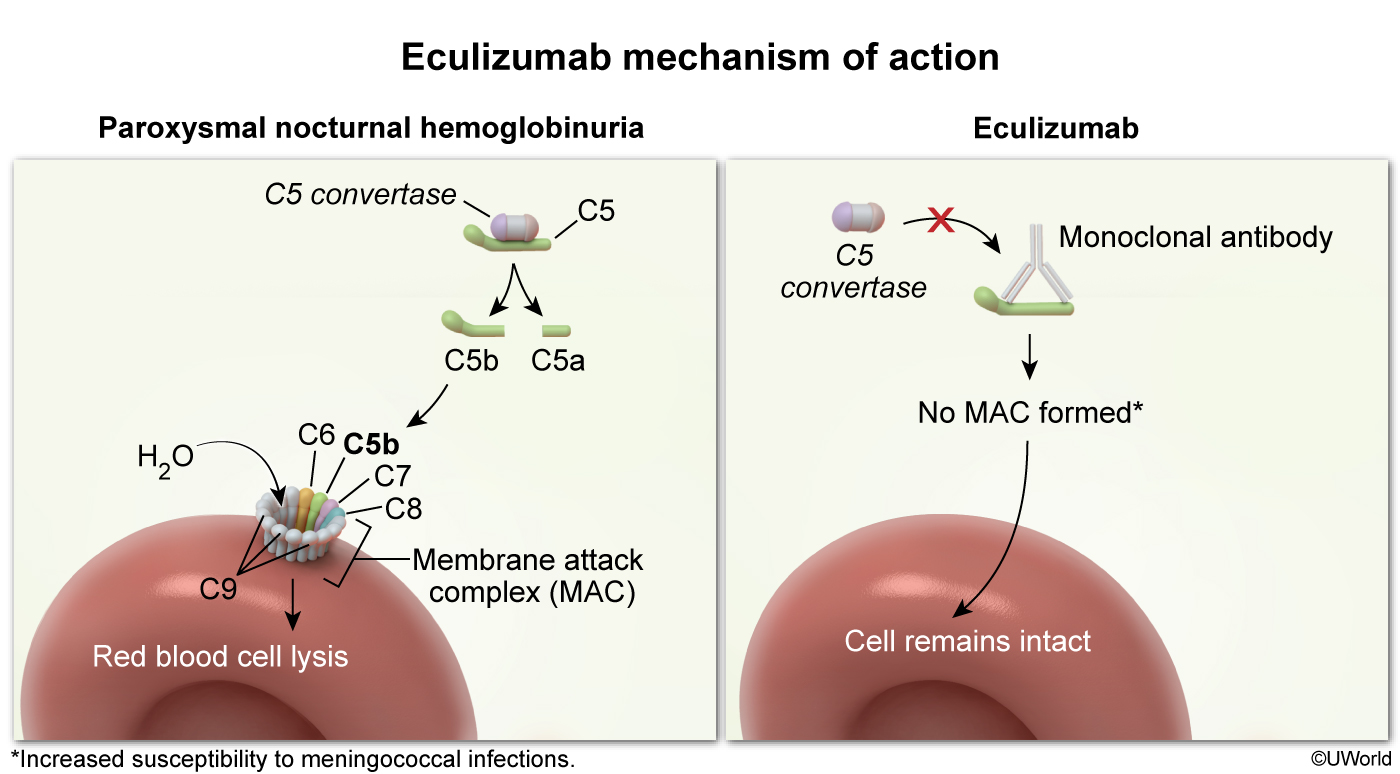
- Treatment: eculizumab (anti-C5 monoclonal antibody) ± allogeneic stem-cell transplant (curative).
Definition
- Paroxysmal Nocturnal Hemoglobinuria (PNH) is a rare acquired clonal disorder of the hematopoietic stem cell.
- Results in production of blood cells that lack GPI-anchored complement-regulatory proteins (CD55 & CD59).
- "Paroxysmal" = comes in attacks. "Nocturnal" = hemolysis worsens at night (mild respiratory acidosis during sleep activates complement). "Hemoglobinuria" = free hemoglobin in urine.
- It is the only acquired intrinsic (membrane) cause of hemolytic anemia — all others (HS, G6PD, sickle cell) are inherited.
Epidemiology
- Rare: ~1–5 cases per million per year.
- Affects young adults (median age 30–40 years).
- No clear sex or ethnic predominance.
- Strong association with aplastic anemia (up to 25% of aplastic anemia patients have a detectable PNH clone) and myelodysplastic syndrome (MDS).
Etiology
- Acquired somatic mutation in the PIGA gene (Phosphatidylinositol Glycan class A) on the X chromosome in a hematopoietic stem cell.
- PIGA is required for the first step of GPI (glycosylphosphatidylinositol) anchor biosynthesis.
- Mutation is not inherited — it is acquired in a single bone-marrow stem cell, which then expands as a clone.
- The mutant clone gains a survival advantage when the marrow is under immune attack (explains the link with aplastic anemia).
Pathophysiology
The whole disease comes from one missing anchor:
- PIGA mutation → cannot make GPI anchor.
- Without the anchor, CD55 (DAF) and CD59 (MIRL) cannot attach to the RBC surface.
- CD55 and CD59 normally inhibit complement (CD59 blocks formation of the MAC, C5b–9).
- Without them, complement is freely activated on the patient's own RBCs → intravascular hemolysis → free hemoglobin in plasma and urine.
The same defect on platelets and WBCs explains the other two pillars:
- Thrombosis – complement-activated platelets release procoagulant microparticles; free hemoglobin scavenges nitric oxide → smooth-muscle constriction and platelet activation.
- Pancytopenia – the underlying stem-cell injury (often linked to aplastic anemia) reduces production of all lineages.
Hemolysis worsens at night because mild respiratory acidosis during sleep activates the alternative complement pathway → classic dark morning urine.
Clinical Features
Think of PNH as a triad:
- 1. Hemolytic anemia (intravascular)
- Fatigue, pallor, jaundice.
- Hemoglobinuria – dark/red/cola-colored urine, classically in the first morning sample.
- Chronic hemolysis → iron deficiency (iron lost in urine as hemosiderin) and folate deficiency.
- 2. Thrombosis (most common cause of death)
- Venous, often at unusual sites:
- Hepatic veins → Budd-Chiari syndrome (very classic exam clue).
- Portal, mesenteric, splenic, cerebral (sagittal sinus) veins.
- Abdominal pain, hepatomegaly, ascites, headache.
- Venous, often at unusual sites:
- 3. Bone marrow failure (pancytopenia)
- Anemia + thrombocytopenia (bleeding) + leukopenia (infections).
- May evolve to aplastic anemia or rarely AML.
Other features: esophageal spasm/dysphagia, erectile dysfunction, and abdominal pain — all from NO depletion by free hemoglobin causing smooth-muscle dystonia.
Diagnosis
Initial labs – show intravascular hemolysis pattern:
- CBC: normocytic anemia (may be microcytic if iron deficient); often pancytopenia.
- ↑ LDH (very high), ↑ indirect bilirubin, ↓ haptoglobin, ↑ reticulocytes.
- Coombs (DAT): NEGATIVE – this distinguishes PNH from autoimmune hemolysis.
- Urine: hemoglobinuria (positive dipstick for blood, no RBCs on microscopy) and chronic hemosiderinuria (specific for chronic intravascular hemolysis).
Confirmatory test – flow cytometry:
- Gold standard: peripheral blood flow cytometry showing absent CD55 and CD59 on RBCs and WBCs.
- FLAER (fluorescent aerolysin) test is even more sensitive – binds GPI anchor directly; absent in PNH cells (especially used on granulocytes/monocytes).
Historical/obsolete tests (know the names — they may appear in older Step 1 questions):
- Ham test – acidified serum induces hemolysis of PNH cells.
- Sugar-water (sucrose) test – low-ionic solution activates complement and lyses PNH cells.
Differential Diagnosis
PNH overlaps with several conditions — separate them using the table below and one or two key clues:
| PNH vs. Other Hemolytic Anemias – Quick Differentiation | ||||
|---|---|---|---|---|
| Feature | PNH | Autoimmune (AIHA) | Hereditary spherocytosis | G6PD deficiency |
| Inheritance | Acquired (PIGA mutation) | Acquired (autoantibody) | Autosomal dominant | X-linked recessive |
| Site of hemolysis | Intravascular | Extravascular (warm) / intra (cold) | Extravascular (spleen) | Both (mostly intra) |
| Coombs (DAT) | Negative | Positive | Negative | Negative |
| Trigger | Spontaneous, sleep, infection | Drugs, lymphoma, SLE | Chronic, splenomegaly | Oxidative stress (fava, drugs) |
| Classic clue | Dark morning urine + Budd-Chiari | Spherocytes + positive Coombs | Spherocytes + ↑ MCHC, ↑ osmotic fragility | Bite cells + Heinz bodies |
Also consider when the picture is mainly pancytopenia:
- Aplastic anemia – hypocellular marrow; can coexist with PNH.
- MDS – dysplastic cells, often older patients.
- Acute leukemia – blasts on smear.
Also see the broader intravascular vs extravascular hemolysis categorization.
Management
Supportive care (every patient):
- Folate supplementation (ongoing high cell turnover).
- Iron replacement (lost in urine).
- Transfusion for symptomatic anemia.
- Anticoagulation for any thrombotic event (and long-term prophylaxis in high-risk patients).
- Vaccination against Neisseria meningitidis, pneumococcus, and H. influenzae at least 2 weeks before starting eculizumab.
Definitive/targeted therapy:
- Eculizumab – humanized monoclonal antibody against C5; blocks formation of MAC → dramatically reduces hemolysis, transfusion need, and thrombosis risk.
- Main adverse effect: Neisseria meningitidis infection (terminal complement is needed to lyse Neisseria) → vaccinate + give penicillin prophylaxis.
- Ravulizumab – longer-acting anti-C5 (similar role).
- Allogeneic hematopoietic stem-cell transplant (HSCT) – the only curative option; reserved for severe disease (bone marrow failure, refractory thrombosis, transformation).
Complications
- Thrombosis – the leading cause of death in PNH. High-risk sites: hepatic (Budd-Chiari), portal, mesenteric, cerebral veins.
- Chronic kidney disease – from renal hemosiderin deposition (chronic hemoglobinuria).
- Pulmonary hypertension – chronic NO depletion.
- Iron-deficiency anemia – chronic urinary iron loss.
- Aplastic anemia – marrow failure may worsen over time.
- Transformation to MDS or AML (uncommon but recognized).
- Meningococcal sepsis – iatrogenic complication of eculizumab therapy.
Mnemonics
| Mnemonic – The Triad "HAT" | |
HAT = the three pillars of PNH:
And remember "55 + 59 = 114 dollars Lost" → lose CD55 and CD59 → lose protection from complement. |
جملة تذكرية |
| Mnemonic – PNH = Please Note Hemolysis | |
|
جملة تذكرية |
Key Points for Exams – نقاط مهمة للامتحانات
- PNH = the only acquired membrane defect causing hemolytic anemia.
- PIGA mutation (X-linked, but somatic — not inherited) → no GPI anchor → no CD55/CD59 → uncontrolled complement → intravascular hemolysis.
- Classic triad: Coombs-negative intravascular hemolysis + atypical thrombosis + pancytopenia.
- Most feared clinical scenario: Budd-Chiari syndrome in a young patient with cytopenias and dark morning urine.
- Labs: ↑ LDH, ↓ haptoglobin, ↑ retics, negative Coombs, urine hemosiderin positive.
- Diagnosis: flow cytometry (CD55/CD59 absent ± FLAER). Ham & sucrose tests are historical.
- Treatment: Eculizumab (anti-C5) — vaccinate against Neisseria meningitidis first. HSCT = cure.
- Main cause of death: thrombosis.
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.