Summary
Microangiopathic hemolytic anemia (MAHA) is a Coombs-negative, normocytic hemolytic anemia characterized by mechanical red blood cell fragmentation in microthrombi-occluded vessels, producing hallmark schistocytes on peripheral smear. All thrombotic microangiopathies present with intravascular hemolysis (elevated LDH, decreased haptoglobin) and thrombocytopenia, but are differentiated by coagulation studies: TTP and HUS demonstrate normal PT/PTT and fibrinogen, whereas DIC presents with prolonged PT/PTT, decreased fibrinogen, and markedly elevated D-dimers due to widespread tissue factor release. TTP stems from ADAMTS13 deficiency (leading to vWF multimers) and features prominent neurological symptoms; treatment is urgent plasma exchange (platelet transfusions are contraindicated). Typical HUS follows Shiga-toxin E. coli O157:H7 gastroenteritis in children, classically causing severe acute kidney injury, and requires supportive care. DIC management relies on treating the underlying trigger (sepsis, trauma, malignancy) and targeted blood product replacement.
Overview
What MAHA is
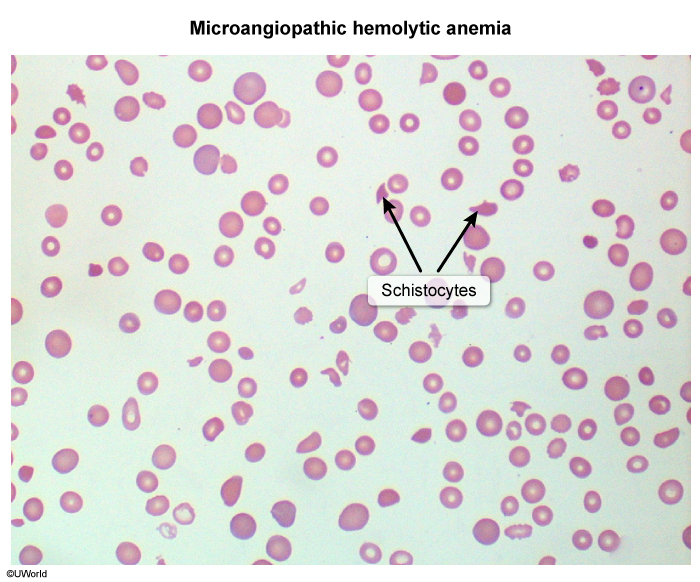
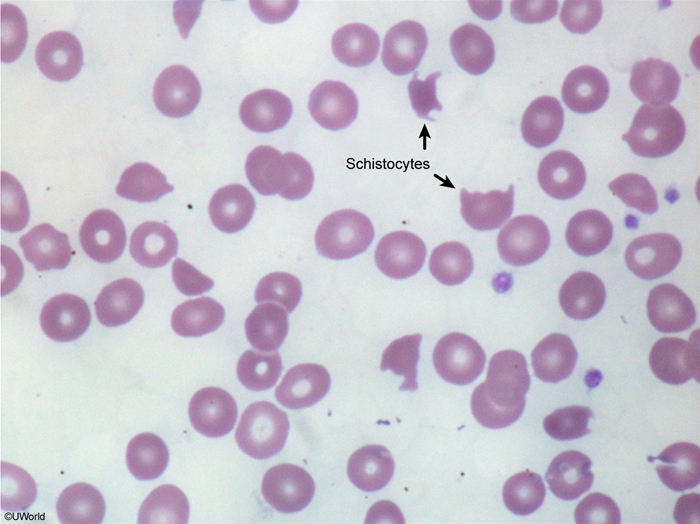
Microangiopathic hemolytic anemia (MAHA) is a normocytic, Coombs-negative hemolytic anemia in which red cells are mechanically sheared as they squeeze past platelet/fibrin thrombi or damaged endothelium in small vessels. The fragments left behind are schistocytes (helmet cells) — the visual hallmark of the disease.
MAHA is the blood-film expression of a thrombotic microangiopathy (TMA). Every TMA shares the same core triad:
- Hemolytic anemia with schistocytes
- Thrombocytopenia (platelets consumed in microthrombi)
- End-organ ischemia (kidney, brain, GI tract)
The three high-yield TMAs are TTP, HUS, and DIC. MAHA also appears in HELLP syndrome, malignant hypertension, scleroderma renal crisis, and mechanical heart-valve hemolysis.
Pathophysiology & Hallmarks
Shared pathophysiology
Picture microvessels plugged with sticky thrombi and fibrin strands. RBCs forced through are cut into fragments, producing two parallel consequences:
- Intravascular hemolysis → ↑ LDH, ↑ indirect bilirubin, ↓ haptoglobin, ↑ reticulocytes, hemoglobinuria.
- Platelet consumption in the thrombi → thrombocytopenia → petechiae, purpura, mucosal bleeding.
What differs is the trigger for the thrombi:
- TTP — ADAMTS13 deficiency → ultra-large vWF multimers → platelet microthrombi (brain > kidney).
- HUS — Shiga toxin (E. coli O157:H7) injures renal endothelium.
- DIC — systemic tissue factor release activates the entire coagulation cascade → bleeding and clotting at once.
The one differentiator
All three present with anemia + thrombocytopenia + schistocytes. The fastest way to separate them is the coagulation panel (PT / PTT / fibrinogen): normal in TTP and HUS, deranged in DIC. Clinical context then splits TTP (adult, neurologic) from HUS (child, bloody diarrhea, AKI).
| Note – ملاحظة | |
|
Every MAHA is Coombs (direct antiglobulin) negative — the hemolysis is mechanical, not autoimmune. Expect the intravascular-hemolysis signature: ↑ LDH, ↑ indirect bilirubin, ↓ haptoglobin, ↑ reticulocytes, plus schistocytes on smear. The schistocyte tells you a thrombotic microangiopathy is happening; the rest of the workup tells you which one. |
ملاحظة |
Thrombotic Thrombocytopenic Purpura (TTP)
Definition
A life-threatening TMA caused by deficiency of ADAMTS13, the metalloprotease that normally cleaves ultra-large von Willebrand factor (vWF) multimers.
Etiology
- Acquired (~95%) — autoantibody against ADAMTS13. Classic patient: adult woman; triggers include HIV, pregnancy, SLE, ticlopidine/clopidogrel, quinine.
- Hereditary (Upshaw–Schulman syndrome) — ADAMTS13 gene mutation; presents in childhood or pregnancy.
Pathophysiology
↓ ADAMTS13 → uncleaved ultra-large vWF multimers remain anchored to endothelium → platelets adhere → platelet-rich microthrombi seed the whole body (brain > kidney). The coagulation cascade is not activated, so PT / PTT / fibrinogen stay normal — only platelets are consumed.
Clinical features — pentad "FAT RN"
| Mnemonic – جملة تذكرية | |
TTP pentad = "FAT RN"
The full pentad is now rare — suspect TTP with just MAHA + thrombocytopenia and no other cause. |
جملة تذكرية |
Key contrasts vs HUS: neurologic involvement is prominent, renal failure is usually mild, and coagulation studies are normal.
Complications
- Stroke, seizures, myocardial ischemia, and death if untreated (mortality ~90%).
- Relapse in ~30–50% of acquired cases.
First-line treatment
- Urgent plasma exchange (plasmapheresis) — removes the autoantibody and replaces ADAMTS13. Start on clinical suspicion; do not wait for the ADAMTS13 result.
- Glucocorticoids in acquired/autoimmune disease.
- Caplacizumab (anti-vWF nanobody) and rituximab (refractory or relapsing disease) as adjuncts.
- Avoid platelet transfusion unless there is life-threatening bleeding.
| فخ امتحاني | |
إعطاء الصفائح الدموية في TTP قد يفاقم من تكوّن الخثرات ويزيد من سوء الحالة، وهو مضاد استطباب إلا في حالات النزيف المهدد للحياة. |
ملاحظة |
Hemolytic Uremic Syndrome (HUS)
Definition
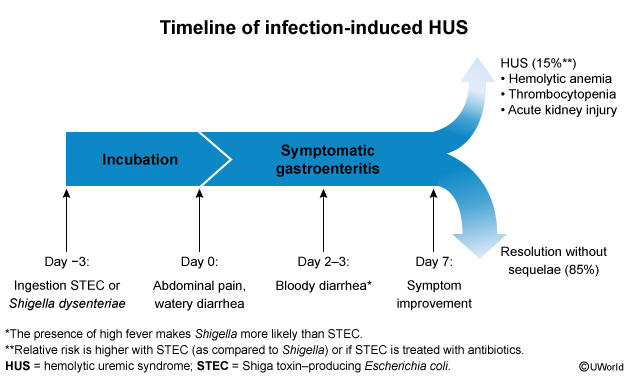
A TMA dominated by acute kidney injury, classically in a young child after bloody diarrhea.
Etiology
- Typical HUS (D+ HUS, ~90%) — Shiga-toxin–producing E. coli O157:H7 (undercooked beef, unpasteurized milk); less often Shigella dysenteriae.
- Atypical HUS (aHUS) — complement dysregulation (e.g., Factor H mutation); no diarrheal prodrome.
Pathophysiology
Shiga toxin enters the blood → binds glycolipid receptors on renal endothelium → endothelial injury → platelet activation → microthrombi concentrated in the kidney → MAHA + thrombocytopenia + AKI.
Clinical features — triad
- Microangiopathic hemolytic anemia (schistocytes)
- Thrombocytopenia
- Acute kidney injury (oliguria, ↑ BUN/Cr, hematuria)
Antecedent bloody diarrhea ~5–10 days earlier in a child <5 years. Neurologic signs are uncommon (contrast with TTP); PT / PTT / fibrinogen are normal.
| Mnemonic – جملة تذكرية | |
HUS triad = "ATR": Anemia (MAHA) + Thrombocytopenia + Renal failure (severe AKI). Organism = E. coli O157:H7 from undercooked hamburger → Shiga toxin. Picture a kid + bloody diarrhea + AKI. |
جملة تذكرية |
Complications
- Chronic kidney disease, hypertension, and end-stage renal failure; rarely colonic necrosis, pancreatitis, or CNS involvement.
First-line treatment
- Supportive: fluid and electrolyte management, RBC transfusion for severe anemia, dialysis for severe AKI.
- Avoid antibiotics and antimotility agents in Shiga-toxin HUS.
- Atypical HUS: eculizumab (anti-C5 complement inhibitor).
| ملاحظة سريرية | |
تجنب المضادات الحيوية في حالات الإسهال الدموي المشتبه بـ E. coli O157:H7، لأنها قد تزيد من إفراز ذيفان الشيغا وترفع خطر الإصابة بـ HUS. |
ملاحظة |
Disseminated Intravascular Coagulation (DIC)
Definition
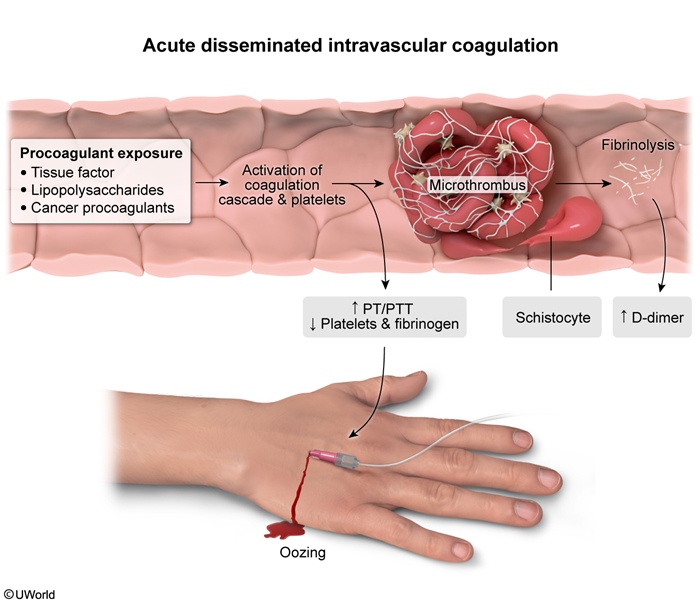
A secondary syndrome of widespread, uncontrolled activation of the coagulation cascade → simultaneous thrombosis and bleeding. Always hunt for the underlying cause.
Etiology — top causes first
The four conditions behind most DIC are Sepsis (especially gram-negative), Trauma / burns, Obstetric emergencies (abruptio placentae, amniotic fluid embolism, retained dead fetus), and Malignancy — notably acute promyelocytic leukemia (APL/M3) and mucinous adenocarcinomas. The full list follows the "STOP Making New Thrombi" mnemonic.
| Mnemonic – جملة تذكرية | |
DIC causes = "STOP Making New Thrombi"
DIC labs = "everything is bad": ↓ platelets, ↓ fibrinogen, ↑ PT, ↑ PTT, ↑↑ D-dimer, schistocytes. |
جملة تذكرية |
Pathophysiology
Massive tissue factor release → systemic thrombin generation → microvascular fibrin deposition → RBC shearing (schistocytes) and organ ischemia. At the same time, platelets and clotting factors are consumed faster than they can be made → bleeding from every site.
Clinical features
- Sick patient (sepsis, post-trauma, post-delivery).
- Bleeding from multiple sites + microthrombotic damage (organ failure, purpura fulminans, digital ischemia).
- Oozing from venipuncture / IV-line sites is a classic clue.
Labs — the deranged panel
- ↓ Platelets
- ↑ PT and PTT (factors consumed)
- ↓ Fibrinogen (consumed)
- ↑↑ D-dimer / fibrin split products (fibrinolysis)
- Schistocytes on smear
This abnormal coagulation panel is what separates DIC from TTP and HUS.
Complications
- Multi-organ failure (ARDS, AKI, hepatic failure), purpura fulminans, digital gangrene, and life-threatening hemorrhage.
First-line treatment
- Treat the trigger — sepsis → antibiotics; obstetric cause → deliver/evacuate; APL → ATRA.
- Blood products for active bleeding: FFP (clotting factors), cryoprecipitate for fibrinogen <100 mg/dL, platelets if <20,000/µL or bleeding, RBCs as needed.
- Heparin — controversial; reserved for predominantly thrombotic or chronic DIC of malignancy.
| Important – فكرة سؤال | |
Acute promyelocytic leukemia (APL, AML-M3) classically presents with DIC: granule-rich promyelocytes release tissue factor → consumptive coagulopathy and life-threatening bleeding. Start all-trans retinoic acid (ATRA) urgently — it both treats the leukemia and resolves the DIC. |
تذكر |
Comparative Diagnosis & Management
Diagnostic approach
Step 1 — Recognize MAHA. CBC shows normocytic anemia + thrombocytopenia; the smear shows schistocytes; hemolysis labs show ↑ LDH, ↑ indirect bilirubin, ↓ haptoglobin, ↑ reticulocytes; the direct Coombs is negative (mechanical, not autoimmune).
Step 2 — Split the three on the coagulation panel.
- Normal PT / PTT / fibrinogen → TTP or HUS (decide by profile: adult + neurologic signs vs child + bloody diarrhea + AKI).
- ↑ PT/PTT, ↓ fibrinogen, ↑↑ D-dimer → DIC.
Step 3 — Confirmatory tests.
- TTP: ADAMTS13 activity <10% confirms; the PLASMIC score stratifies pre-test probability. Treat on suspicion — do not wait for the result.
- HUS: stool culture / Shiga-toxin PCR for E. coli O157:H7.
- DIC: ISTH DIC score (platelets, fibrinogen, D-dimer, PT prolongation).
Master comparison
| TTP vs HUS vs DIC — Master Comparison | |||
|---|---|---|---|
| Feature | TTP | HUS | DIC |
| Typical patient | Adult woman | Child <5 yr after bloody diarrhea | Critically ill (sepsis, obstetric, trauma, malignancy) |
| Trigger | ADAMTS13 deficiency → ultra-large vWF multimers | Shiga toxin (E. coli O157:H7) | Tissue factor release → systemic coagulation |
| Dominant organ | CNS (brain) > kidney | Kidney | Multiple organs |
| Neurologic signs | Prominent (confusion, seizures) | Rare | Variable |
| Renal failure | Mild | Severe (AKI) | Variable |
| Platelets | ↓↓ | ↓ | ↓ |
| PT / PTT | Normal | Normal | ↑↑ Prolonged |
| Fibrinogen | Normal | Normal | ↓ Low |
| D-dimer | Normal / mild ↑ | Normal / mild ↑ | ↑↑↑ Markedly high |
| Peripheral smear | Schistocytes | Schistocytes | Schistocytes |
| First-line treatment | Plasma exchange (urgent) + glucocorticoids ± caplacizumab/rituximab; AVOID platelets | Supportive (fluids, dialysis); NO antibiotics; eculizumab for atypical HUS | Treat underlying cause; FFP, cryoprecipitate, platelets for active bleeding |
Management at a glance
- TTP — urgent plasma exchange + glucocorticoids ± caplacizumab/rituximab; no platelet transfusion unless life-threatening bleeding.
- HUS — supportive (fluids, dialysis for AKI); no antibiotics in Shiga-toxin disease; eculizumab for atypical HUS.
- DIC — treat the cause; replace with FFP / cryoprecipitate / platelets only for active bleeding.
| Important – فكرة سؤال | |
In any patient with MAHA + thrombocytopenia and no other explanation, the safest exam answer is to start empiric plasma exchange while ADAMTS13 is pending — untreated TTP mortality approaches 90%, falling to <20% with prompt exchange. A negative direct Coombs test confirms the hemolysis is mechanical, not autoimmune. |
تذكر |
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.