Summary
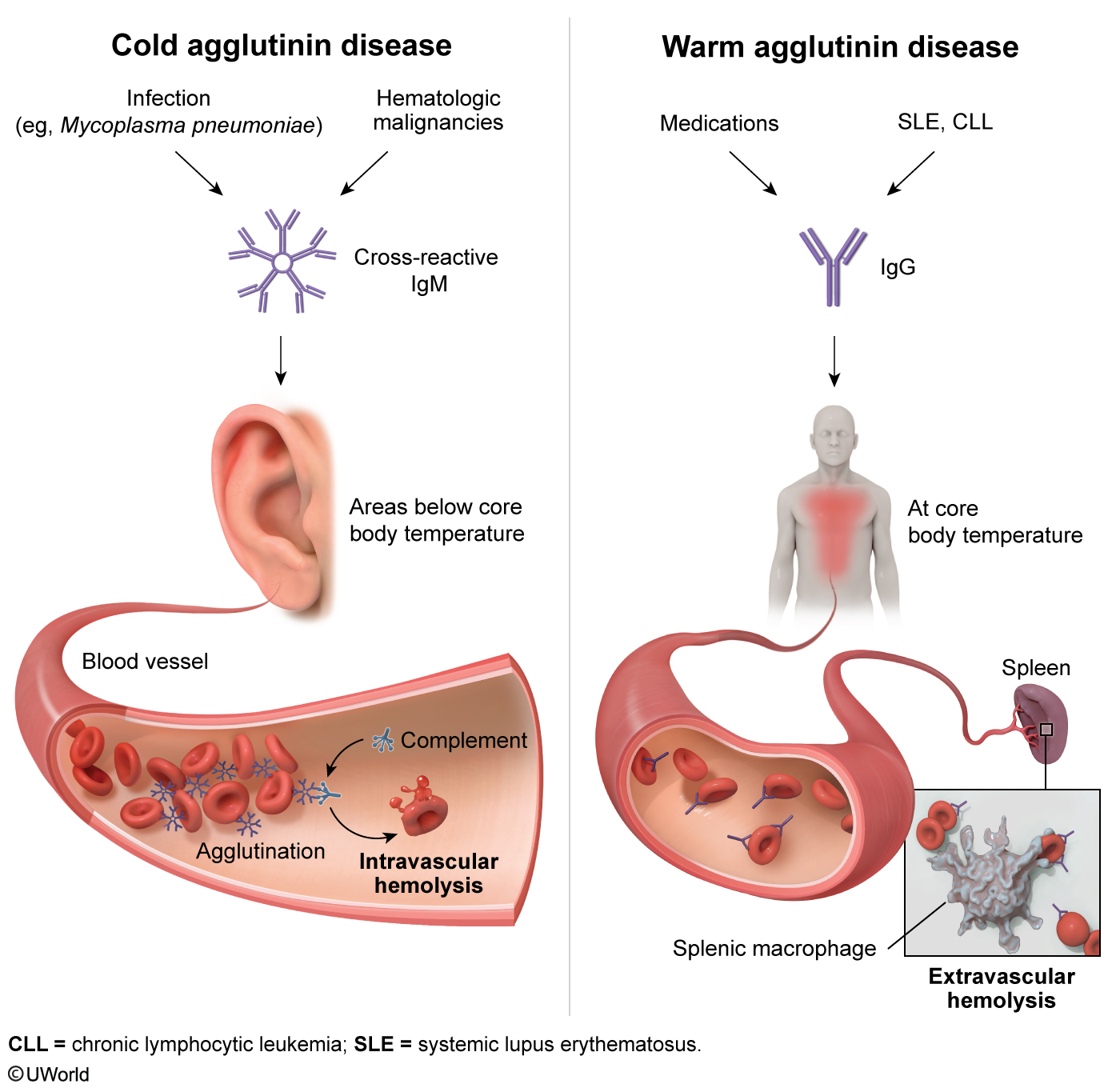
Autoimmune hemolytic anemia (AIHA) presents as an acquired normocytic normochromic anemia (MCV 80–100 fL) characterized by autoantibody-mediated RBC destruction. Pathophysiologically, warm AIHA (~80%) involves IgG autoantibodies binding at 37°C, driving splenic macrophage phagocytosis (extravascular hemolysis), whereas cold AIHA (~20%) involves IgM pentamers binding at 0–4°C to activate complement (C3), causing intravascular and hepatic hemolysis.
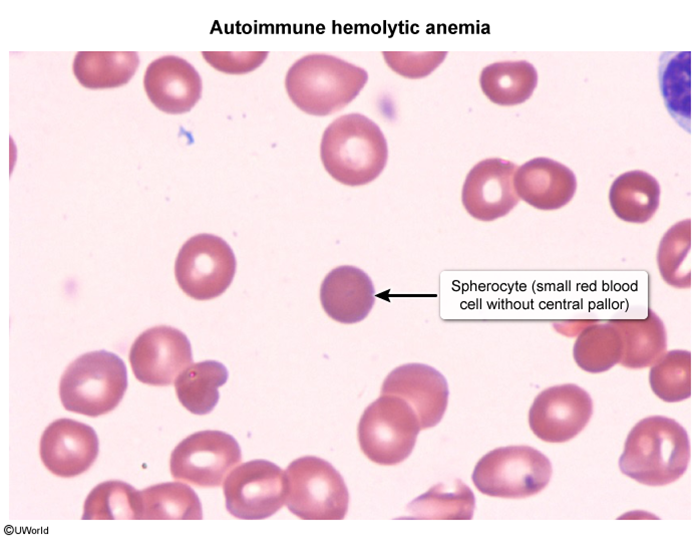
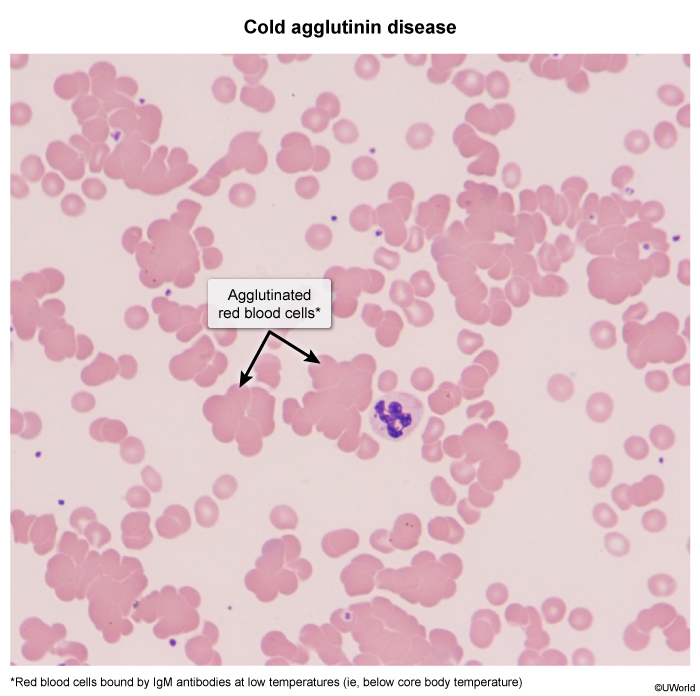
Diagnostic hallmarks on peripheral smear demonstrate spherocytes for warm AIHA and RBC agglutination (often causing artifactual MCV elevation) for cold AIHA. Confirmatory diagnosis requires a positive direct Coombs test (DAT), which isolates anti-IgG (± C3) in warm disease versus anti-C3 only in cold disease. First-line management mandates corticosteroids (± rituximab/splenectomy) for warm AIHA, whereas cold AIHA requires cold avoidance and rituximab (corticosteroids and splenectomy are ineffective).
Overview
Autoimmune hemolytic anemia (AIHA) is an acquired, normocytic normochromic anemia caused by autoantibodies directed against the patient's own RBC surface antigens, leading to premature RBC destruction. The hallmark confirmatory test is a positive direct Coombs test (DAT). AIHA is classified by the temperature at which the antibody best binds RBCs.
Classification
- Warm AIHA (~80%, most common) — IgG antibody, optimal binding at 37°C, extravascular hemolysis (spleen).
- Cold AIHA (~20%) — IgM antibody, optimal binding at 0–4°C, complement-mediated intravascular hemolysis (+ hepatic clearance).
- Mixed type — rare; features of both warm and cold.
- Drug-induced — e.g., α-methyldopa, penicillins, cephalosporins.
Etiology
Warm AIHA
- Primary (idiopathic) — about half of cases.
- Secondary — autoimmune disease (SLE most classic, rheumatoid arthritis); lymphoproliferative disorders (CLL, non-Hodgkin lymphoma); drugs (α-methyldopa, penicillins, cephalosporins, NSAIDs).
Cold AIHA
- Primary — chronic cold agglutinin disease of the elderly.
- Secondary — acute self-limited infections (Mycoplasma pneumoniae, EBV / infectious mononucleosis); lymphoproliferative disorders (Waldenström macroglobulinemia, lymphomas).
For an SLE-associated case, the haematologic profile is summarised in the hematologic manifestations of SLE, where warm AIHA is a recognised complication.
Pathophysiology
Pathophysiology
Warm AIHA — extravascular hemolysis:
- IgG binds RBC surface antigens (mainly Rh) at body temperature.
- The Fc portion of IgG is recognized by splenic macrophages, which partially "bite off" membrane → loss of surface area → spherocyte formation.
- Spherocytes are trapped and destroyed in the spleen → splenomegaly and indirect (unconjugated) hyperbilirubinemia.
Cold AIHA — complement-mediated / intravascular hemolysis:
- IgM binds RBC antigens (anti-I in Mycoplasma; anti-i in EBV) in cold peripheral parts of the body.
- IgM is a potent complement (C3) activator, giving two outcomes:
- Full activation (MAC, C5–C9) → intravascular hemolysis → hemoglobinemia and hemoglobinuria.
- Partial activation (C3b coating) → RBCs cleared by hepatic Kupffer cells.
- The large IgM pentamer also causes RBC agglutination in cold areas → acrocyanosis / Raynaud-like phenomenon.
| Warm vs Cold AIHA — core | |
|
"Warm Goes with Spleen, Cold Makes Cream"
Causes of Cold AIHA — "MEW": Mycoplasma, EBV (mono), Waldenström. |
جملة تذكرية |
| Cold antigen targets | |
|
Mycoplasma → anti-I | EBV (mononucleosis) → anti-i (small "i" for the immature/fetal-type antigen seen in EBV). |
جملة تذكرية |
Diagnostic Approach
Clinical features
Both forms share general hemolysis features: fatigue, pallor, jaundice, dark urine, splenomegaly (especially warm).
- Warm AIHA — more chronic, gradual anemia; jaundice and splenomegaly; may follow a relapsing-remitting course.
- Cold AIHA — symptoms triggered by cold exposure:
- Acrocyanosis — blue/purple discoloration of fingers, toes, ears, nose that improves on warming.
- Raynaud-like phenomenon.
- Episodic dark urine (hemoglobinuria) after cold exposure.
- Post-infectious cases (Mycoplasma, EBV) are usually acute and self-limited.
Spotter sign: a CBC tube left on the bench may show visible RBC clumps in cold AIHA, and the analyzer may report a falsely elevated MCV (clumps counted as one large cell).
Laboratory findings
- Serum: ↓ hemoglobin, ↑ reticulocyte count (compensatory marrow response), ↑ indirect bilirubin, ↑ LDH, ↓ haptoglobin.
- Urine: cold AIHA additionally → hemoglobinemia and hemoglobinuria (intravascular hemolysis).
- Cold-specific: cold agglutinin titer elevated; indirect Coombs may detect free serum IgM.
Peripheral blood smear
- Warm AIHA → spherocytes + polychromasia (reticulocytes); looks identical to hereditary spherocytosis — Coombs distinguishes them.
- Cold AIHA → RBC agglutination (irregular clumps), not the orderly stacked-coin rouleaux of myeloma.
Direct Coombs test (DAT) — the diagnostic test
Detects antibody and/or complement already bound to the patient's RBCs.
- Warm AIHA → DAT positive for anti-IgG (± C3).
- Cold AIHA → DAT positive for anti-C3 only (IgM has detached at lab temperature, but complement remains attached).
| Important – فكرة سؤال | |
|
Interpreting the Direct Coombs Test (DAT):
فخ امتحاني: لو الـ DAT طلع C3 فقط فكّر بـ Cold AIHA؛ ولو طلع anti-IgG فهو Warm AIHA. |
تذكر |
Key differential diagnoses
- Hereditary spherocytosis — spherocytes but Coombs negative; positive family history, ↑ MCHC. See the hereditary spherocytosis reference (negative Coombs) for the features that separate it from warm AIHA.
- G6PD deficiency — bite cells, Heinz bodies; oxidative-stress triggered; Coombs negative. The G6PD deficiency summary lays out the triggers and smear findings.
- Microangiopathic hemolytic anemia (TTP/HUS/DIC) — schistocytes, thrombocytopenia, Coombs negative. Refer to the HUS vs TTP vs ITP differential for the lab pattern.
- Paroxysmal nocturnal hemoglobinuria (PNH) — Coombs negative; flow cytometry shows CD55/CD59 deficiency.
- Hemolytic transfusion reaction — Coombs may be positive but in the setting of recent transfusion.
- Multiple myeloma rouleaux — stacked-coin appearance, NOT agglutination; no hemolysis labs.
| Important – فكرة سؤال | |
|
Spherocytes on smear — two differentials:
فخ امتحاني: الـ spherocytes موجودة في الحالتين، والفيصل هو الـ Coombs: سلبي في hereditary spherocytosis وإيجابي في warm AIHA. |
تذكر |
Management & Key Complications
Warm AIHA — treatment
- Step 1 — Corticosteroids (first-line): prednisone 1 mg/kg/day PO; effective in ~70–80%. Taper once hemoglobin recovers.
- Step 2 — Rituximab: if steroid-refractory or relapsing.
- Step 3 — Splenectomy: for steroid- and rituximab-refractory cases (removes the main site of RBC destruction).
- Step 4 — Other immunosuppressants: azathioprine, cyclophosphamide, mycophenolate.
- Treat the underlying cause — stop the offending drug; treat SLE/CLL.
- Folate supplementation (high RBC turnover).
- Transfusion only for life-threatening anemia (crossmatch is difficult — warm the patient and give the "least incompatible" unit).
Cold AIHA — treatment
- Cold avoidance — cornerstone: keep extremities warm; warm all IV fluids and blood products.
- Treat the underlying cause: Mycoplasma/EBV cases usually self-resolve.
- Rituximab: first-line drug therapy for chronic/severe cold agglutinin disease.
- Plasmapheresis: useful in acute severe hemolysis (removes circulating intravascular IgM).
- Steroids and splenectomy are NOT effective — hemolysis is hepatic/intravascular, and IgM is not steroid-responsive.
| Important – فكرة سؤال | |
Treatment dichotomy (classic exam trap):
فخ امتحاني: الستيرويد والـ splenectomy ينفعان في الـ Warm فقط؛ في الـ Cold الأساس تجنّب البرد + rituximab، والستيرويد لا ينفع. |
تذكر |
Key complications
- Severe symptomatic anemia — fatigue, dyspnea, high-output heart failure in the elderly.
- Hemolytic crisis — especially cold AIHA after cold exposure.
- Venous thromboembolism (VTE) — AIHA is a recognized hypercoagulable state.
- Pigment (bilirubin) gallstones — from chronic indirect hyperbilirubinemia.
- Transfusion difficulties — autoantibodies interfere with crossmatching.
- Post-splenectomy (warm AIHA) — risk of encapsulated-organism infection; vaccinate against S. pneumoniae, H. influenzae, N. meningitidis.
- Long-term steroid toxicity — osteoporosis, hyperglycemia, infection, Cushingoid features.
High-Yield Comparison & Exam Pearls
This master table consolidates warm vs cold AIHA across every tested domain — antibody, temperature, hemolysis site, causes, smear, Coombs, and treatment.
| Warm vs Cold AIHA — Master Comparison | ||
|---|---|---|
| Domain | Warm AIHA | Cold AIHA |
| Antibody class | IgG (warm-reactive) | IgM (cold-reactive, pentamer) |
| Optimal binding temperature | 37°C (body temperature) | 0–4°C (cold extremities) |
| Complement role | Usually minimal (± C3) | Strong complement (C3) activator |
| Site of hemolysis | Extravascular — spleen | Intravascular + extravascular (hepatic Kupffer cells) |
| Frequency | ~80% (most common) | ~20% |
| Peripheral smear | Spherocytes + polychromasia | RBC agglutination (clumping) |
| Direct Coombs (DAT) | Anti-IgG (± C3) | Anti-C3 only |
| Typical causes | Idiopathic, SLE, CLL/lymphoma, α-methyldopa, penicillins | Mycoplasma (anti-I), EBV (anti-i), Waldenström, lymphoma |
| Key clinical clue | Splenomegaly, chronic jaundice | Acrocyanosis, Raynaud-like, cold-triggered hemoglobinuria |
| First-line treatment | Corticosteroids (prednisone 1 mg/kg/day) | Cold avoidance + rituximab |
| Refractory / second-line | Rituximab, then splenectomy | Plasmapheresis (acute); steroids & splenectomy NOT effective |
| Key Points for Exams – نقاط مهمة للامتحانات | |
|
ملاحظة |
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.