Summary
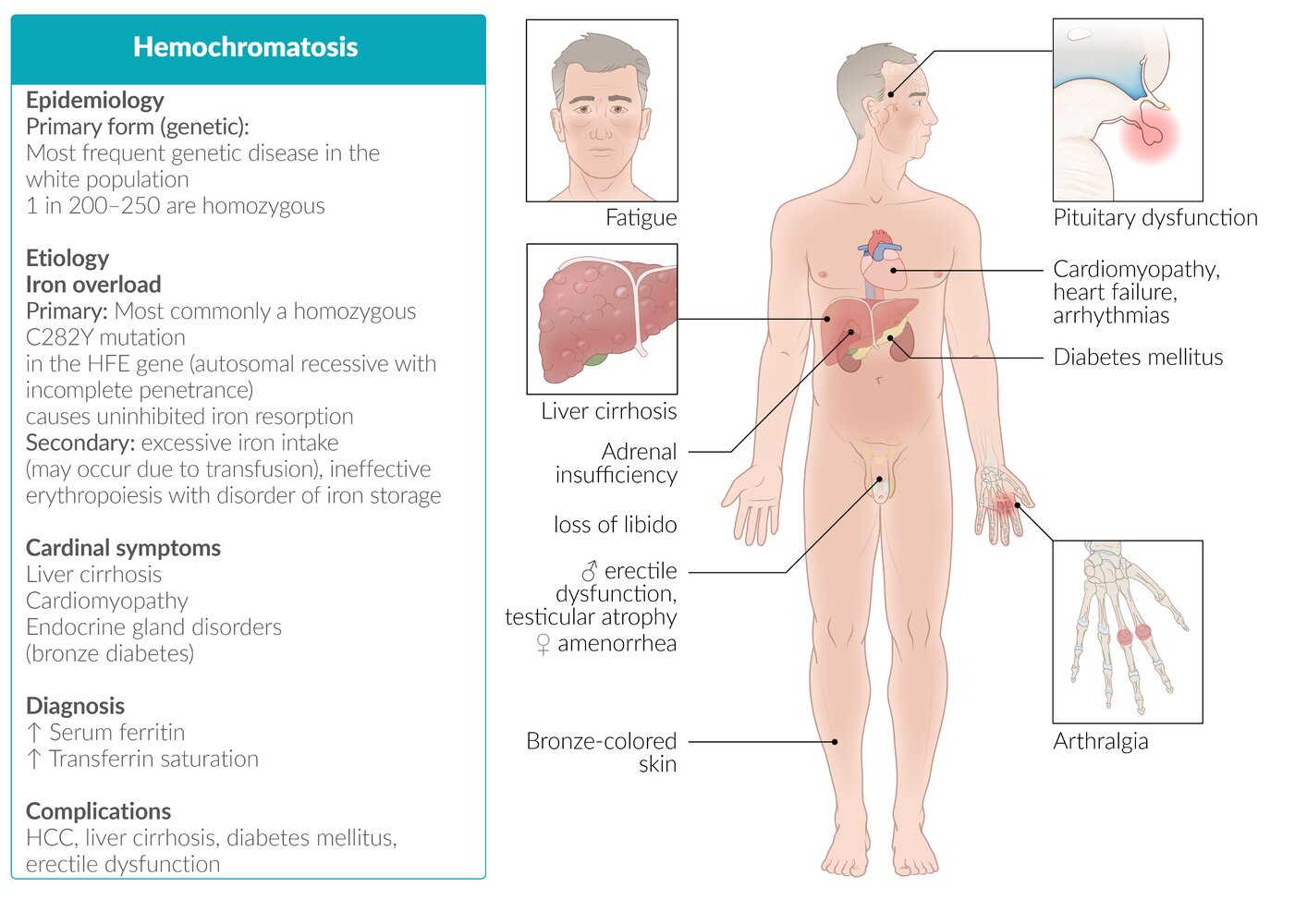
Hemochromatosis is an iron overload disorder characterized by excessive intestinal iron absorption leading to tissue deposition and organ damage. The condition is most commonly hereditary (HFE gene mutations) and presents with the classic triad of cirrhosis, diabetes mellitus ("bronze diabetes"), and skin hyperpigmentation. Early diagnosis through iron studies (elevated transferrin saturation >45% and ferritin) is crucial as treatment with phlebotomy can prevent complications. Without treatment, patients face serious complications including hepatocellular carcinoma, heart failure, and arthropathy.
Definition
- Iron overload disorder caused by increased intestinal iron absorption
- Most common genetic metabolic disorder in people of Northern European descent
- Total body iron exceeds 20g (normal: 3-4g) leading to tissue damage
- Two main types:
- Hereditary hemochromatosis (HH): Autosomal recessive, HFE gene mutations (C282Y most common)
- Secondary hemochromatosis: Due to chronic transfusions, hemolytic anemias, or excessive iron intake
Pathophysiology
HFE protein normally regulates iron absorption by sensing iron stores. Mutations lead to:
- Falsely detected low iron → Decreased hepcidin synthesis by hepatocytes
- Increased DMT1 expression on enterocytes → Enhanced iron absorption
- Increased ferroportin activity → More iron enters circulation
- Progressive iron accumulation in organs (liver, heart, pancreas, pituitary, joints)
shows the mechanism of iron overload in hemochromatosis.
Clinical Features
Remember the classic presentation: "Bronze diabetes with arthritis"
| Clinical Manifestations of Hereditary Hemochromatosis | |
|---|---|
| System | Manifestations |
| Skin |
|
| Musculoskeletal |
|
| Gastrointestinal |
|
| Endocrine |
|
| Cardiac |
|
| MCP = metacarpophalangeal | |
| Important – فكرة سؤال | |
| Men present earlier than women (menstruation is protective). Look for a middle-aged man with diabetes + arthritis + elevated liver enzymes = Think hemochromatosis! | تذكر |
Diagnosis
Two-step approach:
- Screen for iron overload:
- Transferrin saturation >45% (best screening test)
- Serum ferritin elevated (>200 ng/mL women, >300 ng/mL men)
- Confirm diagnosis:
- HFE genetic testing (C282Y homozygous most common)
- MRI liver/heart for iron quantification
- Liver biopsy (rarely needed) - shows iron deposition with Prussian blue stain
demonstrates characteristic arthropathy changes.
| Note | |
| Ferritin alone is not specific - it's an acute phase reactant. Always check transferrin saturation! | ملاحظة |
Differential Diagnosis
- Secondary iron overload: Chronic transfusions, thalassemia, sideroblastic anemia
- Wilson disease: Copper overload, Kayser-Fleischer rings, neuropsychiatric symptoms
- Porphyria cutanea tarda: Photosensitive skin lesions, bullae on hands ()
- Chronic liver disease: Alcohol, NAFLD, viral hepatitis
Treatment
Goal: Reduce iron stores and prevent complications
- First-line: Phlebotomy
- Initial: Weekly removal of 500mL blood until ferritin normalizes
- Maintenance: Every 2-4 months to keep ferritin 50-100 ng/mL
- Urgent if ferritin >1000 ng/mL (high risk for organ damage)
- Alternative (if phlebotomy contraindicated):
- Iron chelation therapy (deferoxamine, deferasirox)
- Supportive measures:
- Avoid iron supplements, vitamin C
- Limit alcohol (accelerates liver damage)
- Screen for complications (HCC surveillance if cirrhosis)
Complications
- Hepatocellular carcinoma - 20-fold increased risk (main cause of death)
- Heart failure - from cardiomyopathy
- Cirrhosis - if untreated
- Diabetes mellitus - may require insulin
- Arthropathy - progressive, may not improve with treatment
- Infections - increased susceptibility to Listeria, Vibrio vulnificus, Yersinia
Prognosis
- Normal life expectancy if treated before cirrhosis develops
- Phlebotomy improves fatigue, liver enzymes, and cardiac function
- Arthropathy and hypogonadism may persist despite treatment
- Cirrhosis and diabetes are usually irreversible
High-Yield Points for Exams
| Hemochromatosis – Quick Review | |
|---|---|
| Feature | Details |
| Classic Triad | Cirrhosis + Diabetes + Skin pigmentation |
| Best Screening Test | Transferrin saturation > 45% |
| Confirmatory Test | HFE genetic testing (C282Y mutation) |
| Treatment | Phlebotomy (urgent if ferritin > 1000) |
| Most Common Cause of Death | Hepatocellular carcinoma |
| Arthropathy Location | 2nd & 3rd MCP joints |
| MCP = metacarpophalangeal | |
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.