شرح المدرسين

Summary
Non-megaloblastic macrocytic anemia is defined as an elevated mean corpuscular volume (MCV > 100 fL, typically 100–110 fL) with intact DNA synthesis. Pathophysiology involves red blood cell membrane lipid expansion (excess cholesterol and phospholipids) or a young erythroid population (reticulocytosis). Major causes include chronic liver disease, chronic alcohol use disorder, reticulocytosis (hemolysis or hemorrhage), hypothyroidism, and myelodysplastic syndrome (MDS).
Peripheral blood smear reveals round macrocytes (or target cells/acanthocytes in hepatic disease) and notably lacks hypersegmented neutrophils or macro-ovalocytes.
Diagnosis relies on confirming normal serum B12 and folate levels to exclude megaloblastic anemia, alongside liver function tests, TSH, and a reticulocyte count. Management centers on treating the underlying etiology (e.g., alcohol cessation, thyroid replacement); administer thiamine before glucose or folate in patients with alcohol use disorder.
Overview & Pathophysiology
Non-megaloblastic macrocytic anemia = anemia with MCV > 100 fL but normal DNA synthesis. Unlike megaloblastic anemia (B12/folate deficiency), the macrocytosis arises from one of two core mechanisms:
- Excess membrane lipid — cholesterol and phospholipids deposit on the RBC membrane → increased surface area → large, round cells.
- Young red cell population (reticulocytosis) — reticulocytes are ~20% larger than mature RBCs → when released in large numbers, the average MCV rises.
Top 3 Causes
- Chronic liver disease (most common clinically): the diseased liver alters lipid metabolism → cholesterol and phospholipids deposit on the RBC membrane → increased surface area → round macrocytes. Selective cholesterol excess → target cells (codocytes). End-stage liver disease → acanthocytes (spur cells), which are trapped in the spleen and hemolyzed.
- Chronic alcohol use: direct toxic effect of ethanol/acetaldehyde on erythroid precursors in the bone marrow. Macrocytosis can appear even without anemia and with normal B12/folate. Alcoholics frequently develop coexisting folate deficiency (poor diet), producing a mixed megaloblastic/non-megaloblastic picture.
- Reticulocytosis: reticulocytes are ~20% larger than mature RBCs. When the marrow responds to hemolysis or acute blood loss, the average cell size rises. This is physiologic, appropriate macrocytosis — not a bone marrow disease.
Other Notable Causes
- Hypothyroidism — mild macrocytosis; corrects with thyroid hormone replacement.
- Drugs — zidovudine (AZT) (most classic drug cause), hydroxyurea.
- Myelodysplastic syndrome (MDS) — elderly patient with pancytopenia + macrocytosis; risk of AML transformation.
See the Common Causes of Macrocytic Anemia (MCV >100 μm³) for the full differential organized by megaloblastic vs. non-megaloblastic mechanism.
| "FAT RBC" — Non-megaloblastic Macrocytic Anemia Causes | |
|
جملة تذكرية |
| ملاحظة سريرية – Clinical Note | |
فقر الدم كبير الكريات غير الميغالوبلاستي يعني أن MCV > 100 fL ولكن بدون اضطراب في تصنيع DNA — أي لا يوجد hypersegmented neutrophils ولا نقص في B12 أو الفولات. أهم ثلاثة أسباب: أمراض الكبد، الكحول، وارتفاع الـ reticulocytes. |
ملاحظة |
| MCV as a Screening Marker — فكرة سؤال | |
Macrocytosis from alcohol can appear even without anemia and with normal B12/folate. An incidentally elevated MCV on routine CBC is one of the most sensitive laboratory markers of chronic alcohol use — more sensitive than GGT or AST:ALT ratio. Expect this as a "next best step" question. |
تذكر |
Diagnostic Approach & Clinical Features
The workup of macrocytic anemia follows a systematic 4-step approach. The algorithm below outlines the MCV- and reticulocyte-based branching logic:
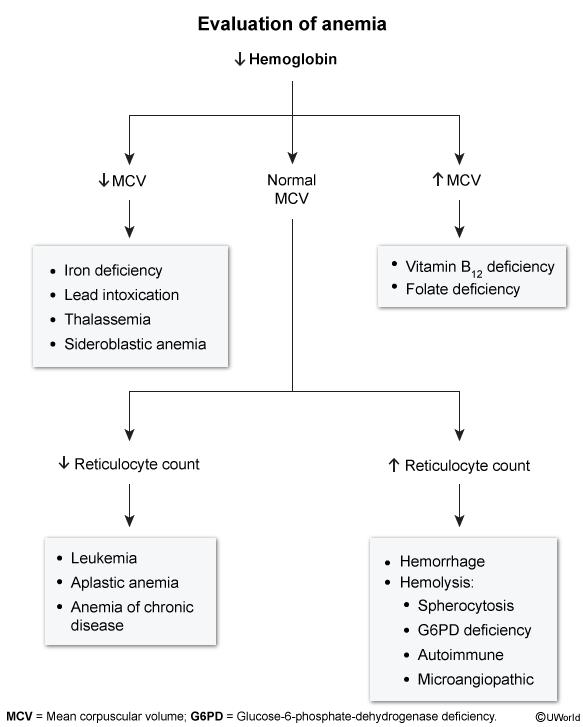
Step 1 — Confirm macrocytic anemia
- CBC: Hb low, MCV > 100 fL.
- MCV is usually mildly elevated (100–110 fL) in non-megaloblastic causes. Values > 115 fL strongly favor megaloblastic anemia.
Step 2 — Reticulocyte count
- High reticulocytes → hemolysis or acute blood loss (the young cells themselves raise the MCV).
- Low / normal reticulocytes → think liver disease, alcohol, hypothyroidism, drugs, MDS.
Step 3 — Peripheral blood smear
The smear rapidly separates non-megaloblastic from megaloblastic causes and narrows the etiology:
- Round macrocytes → non-megaloblastic. Oval macrocytes (macro-ovalocytes) → megaloblastic.
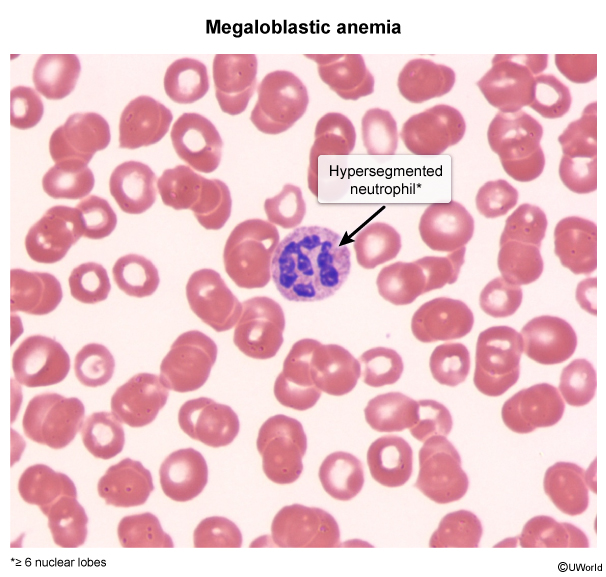
- No hypersegmented neutrophils → confirms non-megaloblastic mechanism.
- Target cells (codocytes) → chronic liver disease (also thalassemia, post-splenectomy).
- Acanthocytes (spur cells) → end-stage liver disease; indicates poor prognosis (spur-cell hemolytic anemia).
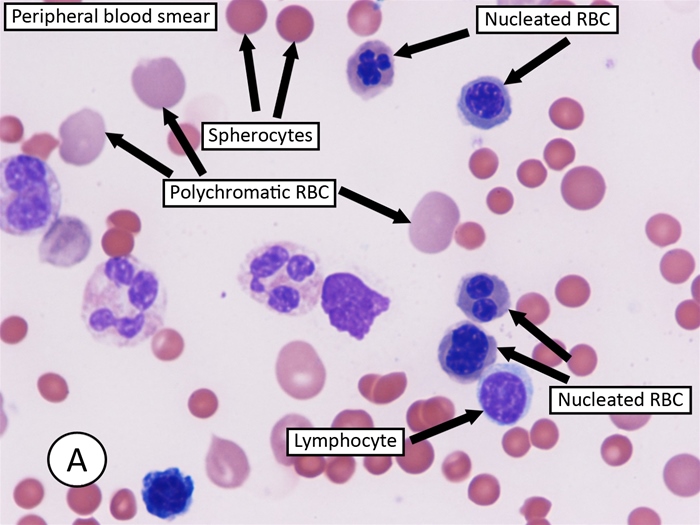
- Polychromasia → large blue-grey RBCs (reticulocytes); indicates active marrow response to hemolysis or bleeding.
The image below demonstrates a peripheral smear in hemolytic anemia with prominent reticulocytosis and spherocytes:
Step 4 — Cause-specific workup
- B12 and folate levels — always check to rule out megaloblastic anemia (must be normal in pure non-megaloblastic).
- LFTs (AST, ALT, bilirubin, albumin, INR) — liver disease. AST:ALT ratio ≥ 2 + elevated GGT → alcoholic liver disease. Refer to the Clinical Features of Alcoholic Hepatitis for the complete diagnostic pattern.
- TSH — hypothyroidism.
- Hemolysis screen: LDH↑, indirect bilirubin↑, haptoglobin↓, Coombs test. See the Causes of Hemolysis: Intravascular vs. Extravascular for the classification of hemolytic mechanisms.
- Bone marrow biopsy — if MDS suspected (elderly + unexplained pancytopenia + dysplastic cells).
Clinical Clues by Cause
- Liver disease: jaundice, ascites, spider angiomas, palmar erythema, splenomegaly.
- Alcoholism: heavy drinking history, signs of liver disease, peripheral neuropathy (from thiamine deficiency, not B12).
- Hemolysis: jaundice, dark urine, splenomegaly, family history of anemia.
- Hypothyroidism: cold intolerance, constipation, weight gain, bradycardia, dry skin.
- MDS: elderly, fatigue, bleeding tendency, recurrent infections (pancytopenia).
Key negative findings: no neurologic symptoms (differentiates from B12 deficiency) and no glossitis (seen in megaloblastic anemia).
| Absence of Hypersegmented Neutrophils — فكرة سؤال | |
The single most useful negative finding on the smear: absence of hypersegmented neutrophils. If hypersegmented neutrophils (≥5 lobes) ARE present, the anemia is megaloblastic — even if the patient has liver disease or drinks alcohol. Their absence confirms a non-megaloblastic mechanism. فخ امتحاني: إذا وجدت hypersegmented neutrophils عند مريض كحولي = السبب megaloblastic (نقص فولات) حتى لو عنده كبد مريض. |
تذكر |
Megaloblastic vs. Non-Megaloblastic: Key Comparison
This is the most commonly tested distinction on board exams. Master the table below — every row is a potential exam question:
| Megaloblastic vs. Non-Megaloblastic Macrocytic Anemia | ||
|---|---|---|
| Feature | Megaloblastic | Non-Megaloblastic |
| Mechanism | Impaired DNA synthesis | Membrane lipid excess OR young RBCs (reticulocytes) |
| Common causes | B12 / folate deficiency; antimetabolite drugs | Liver disease, alcohol, reticulocytosis, hypothyroidism |
| MCV | Often >115 fL | Usually 100–110 fL |
| RBC morphology | Oval macrocytes (macro-ovalocytes) | Round macrocytes |
| Hypersegmented neutrophils (≥5 lobes) | Present — hallmark finding | Absent |
| Reticulocyte count | Low (ineffective erythropoiesis) | Variable — high if hemolysis/bleeding |
| LDH / indirect bilirubin | Markedly elevated (intramedullary hemolysis) | Normal or mildly elevated |
| Neurologic symptoms | Yes (subacute combined degeneration in B12 deficiency) | No |
| Treatment | Replace B12 and/or folate | Treat underlying cause |
The paired smear comparison below demonstrates the key morphologic distinction — hypersegmented neutrophils with oval macrocytes (megaloblastic) versus spherocytes with polychromatic reticulocytes and round macrocytes (non-megaloblastic):
See the Folate Deficiency Anemia: Etiology, Clinical Features, Lab Findings, and Treatment for a detailed review of the most common megaloblastic cause for comparison.
| Mixed Picture Trap — فخ امتحاني | |
|
A patient with chronic alcohol use can have both non-megaloblastic macrocytosis (direct ethanol toxicity) and megaloblastic macrocytosis (folate deficiency from poor diet) simultaneously. Always check B12 and folate levels even when the clinical picture "obviously" points to alcohol. المريض الكحولي قد يكون عنده سببين لارتفاع MCV في نفس الوقت: تأثير الكحول المباشر + نقص الفولات. لذلك يجب فحص B12 و folate دائماً حتى لو السبب واضح. |
تذكر |
Management by Etiology
There is no specific drug for non-megaloblastic macrocytic anemia. Management is directed entirely at the underlying cause:
- Liver disease: treat the underlying hepatic condition (stop alcohol, antiviral therapy for hepatitis, manage cirrhosis complications). Macrocytosis typically persists as long as liver disease is active. Refer to the Laboratory Abnormalities in Liver Dysfunction for the key parameters to monitor during follow-up.
- Alcohol: abstinence is the definitive treatment. MCV normalizes over ~2–4 months after cessation.
- Give thiamine 100 mg IV/IM first (to prevent Wernicke encephalopathy) before giving glucose or folate.
- Supplement folic acid 1 mg PO daily if deficient — common in malnourished alcoholics.
- Reticulocytosis (hemolysis / blood loss): identify and treat the cause of hemolysis or bleeding. Macrocytosis resolves once the marrow response settles.
- Hypothyroidism: levothyroxine replacement; MCV normalizes with adequate thyroid hormone levels.
- Drug-induced: discontinue or dose-reduce the offending agent if clinically feasible. If the drug is essential (e.g., AZT for HIV, hydroxyurea for sickle cell), macrocytosis is accepted as a known side effect and monitored.
- MDS: hematology referral — options include supportive care (transfusions, erythropoietin), hypomethylating agents (azacitidine 75 mg/m² SC/IV daily × 7 days per 28-day cycle; decitabine), or allogeneic stem-cell transplant for eligible patients.
Supportive Measures
- Transfusion: only if symptomatic anemia or Hb < 7 g/dL.
- Always check and replace folate in alcoholics — even if the primary mechanism is non-megaloblastic, coexisting folate deficiency is common.
- Nutritional counseling and alcohol cessation support for at-risk patients.
Complications
Complications arise from the underlying disease, not the mild anemia itself:
- Liver disease: progression to cirrhosis → portal hypertension, variceal bleeding, hepatic encephalopathy, hepatocellular carcinoma. Spur-cell hemolytic anemia (acanthocyte-mediated) carries a particularly poor prognosis. See the Clinical Features of Cirrhosis for the full spectrum of cirrhotic complications.
- Alcohol: Wernicke-Korsakoff syndrome, pancreatitis, alcoholic cardiomyopathy, progression to alcoholic cirrhosis.
- Chronic hemolysis: pigment gallstones (calcium bilirubinate), splenomegaly, iron overload if repeatedly transfused.
- MDS → AML: transformation to acute myeloid leukemia in ~30% of cases — one of the most commonly tested board facts.
Key Points for Exams – نقاط مهمة للامتحانات
Key Points for Exams – نقاط مهمة للامتحانات
- Non-megaloblastic macrocytic anemia = MCV > 100 fL + normal DNA synthesis + round macrocytes + no hypersegmented neutrophils.
- Top 3 causes: liver disease, alcohol, reticulocytosis (remember: "FAT RBC").
- Elevated MCV is one of the most sensitive screening markers of chronic alcohol use — can occur even without anemia or B12/folate deficiency.
- Always check B12 and folate to rule out a coexisting megaloblastic component, especially in alcoholics (mixed picture is common).
- MCV > 115 fL → strongly favors megaloblastic; 100–110 fL → favors non-megaloblastic.
- Smear clues: target cells → liver disease; acanthocytes → end-stage liver; polychromasia → reticulocytosis.
- No neurologic symptoms and no glossitis — distinguishes from B12 deficiency.
- MDS → AML transformation in ~30% of cases.
- Treatment = treat the underlying cause. In alcoholics: thiamine first, then folate if deficient.
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.