شرح المدرسين

Summary
Megaloblastic anemia is a macrocytic anemia (MCV > 100) caused by impaired DNA synthesis, most commonly secondary to Vitamin B12 or Folate deficiency. Patients typically present with anemia symptoms, glossitis, and classic peripheral smear findings of macro-ovalocytes and hypersegmented neutrophils. While both deficiencies share hematologic features, B12 deficiency uniquely presents with neurological impairment (subacute combined degeneration) due to defective myelination.
Diagnosis is confirmed by elevated homocysteine levels, with elevated methylmalonic acid (MMA) specifically distinguishing B12 deficiency from folate deficiency. Treatment requires targeted vitamin replacement; however, folate monotherapy must never be given without ruling out B12 deficiency to prevent progressive, irreversible neurological damage.
Overview
Megaloblastic anemia is a macrocytic anemia (MCV > 100 fL) caused by impaired DNA synthesis in hematopoietic precursors, most commonly due to vitamin B12 (cobalamin) or folate (B9) deficiency. The core cellular defect is nuclear–cytoplasmic asynchrony — the nucleus matures slowly while the cytoplasm develops normally — producing large, fragile megaloblasts that undergo intramedullary hemolysis (ineffective erythropoiesis) with mild ↑ LDH and ↑ indirect bilirubin.
Pathophysiology
Biochemical basis — why DNA synthesis fails
Both vitamins converge on synthesis of thymidine (dTMP), an essential DNA nucleotide:
- Folate (as 5,10-methylene-THF) donates a methyl group: dUMP → dTMP via thymidylate synthase
- B12 is required to regenerate active THF from 5-methyl-THF via the homocysteine → methionine reaction (enzyme: methionine synthase)
- Without either vitamin → insufficient thymidine → impaired DNA replication → delayed nuclear maturation in all rapidly dividing cells (bone marrow, GI epithelium)
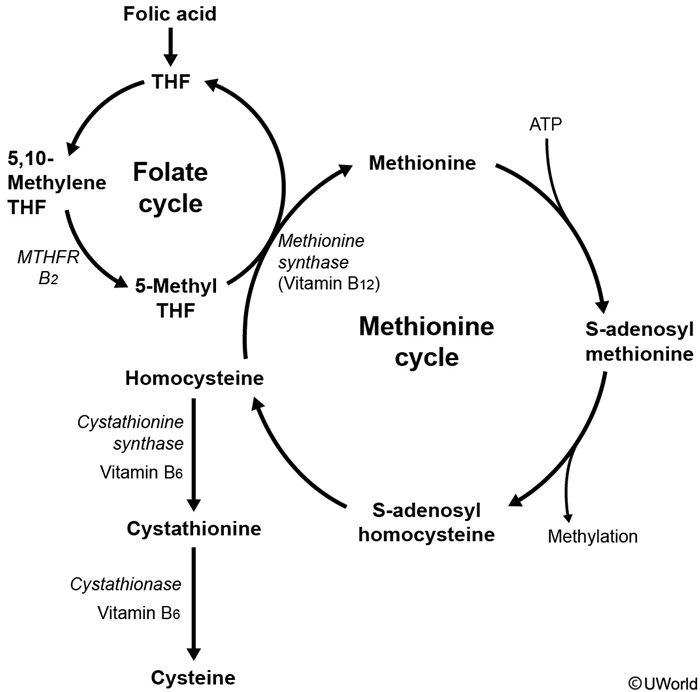
| The Methyl-Folate Trap — ملاحظة | |
| In B12 deficiency, folate gets "trapped" as 5-methyl-THF because B12 is required to convert it back to THF (via methionine synthase). This creates a functional folate deficiency even when folate stores are adequate — explaining why both deficiencies produce the same megaloblastic picture. | ملاحظة |
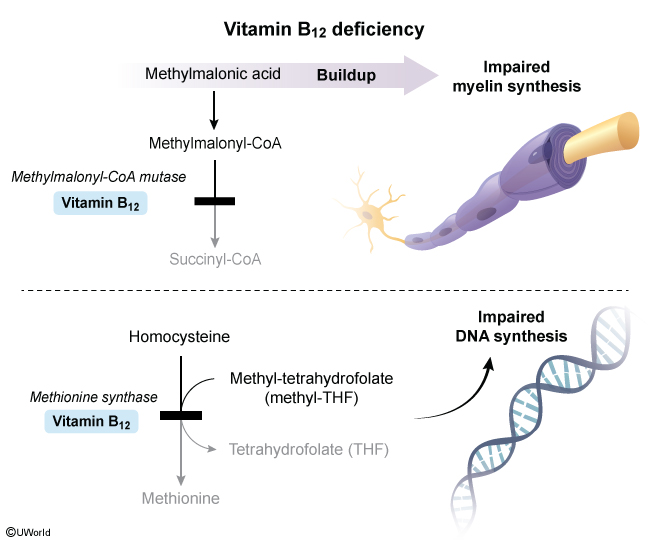
Why only B12 causes neurologic damage
B12 has a second enzymatic role — cofactor for methylmalonyl-CoA mutase (methylmalonyl-CoA → succinyl-CoA):
- In B12 deficiency → ↑ methylmalonic acid (MMA) → abnormal odd-chain fatty acids incorporated into myelin → demyelination
- Affected tracts: dorsal columns, lateral corticospinal tracts, spinocerebellar tracts → subacute combined degeneration
- Folate has no role in this pathway → no neurologic symptoms in isolated folate deficiency
| B12 Neurologic Features — "3 D's of B12" | |
| • Dementia (megaloblastic madness) • Dorsal column dysfunction (↓ vibration, ↓ proprioception, + Romberg) • Degeneration of lateral corticospinal tracts (spasticity, + Babinski) |
جملة تذكرية |
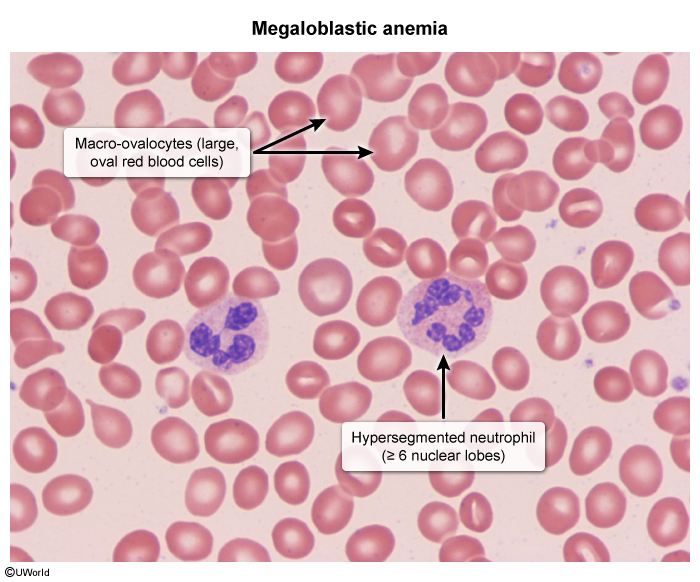
Hallmark peripheral smear findings shared by both deficiencies: macro-ovalocytes and hypersegmented neutrophils (≥ 5 lobes) — the earliest and most specific morphologic clue to megaloblastic anemia.
High-Yield Etiologies
The key is knowing which patient gets which deficiency. Focus on 3 high-yield causes per vitamin.
B12 deficiency — top causes
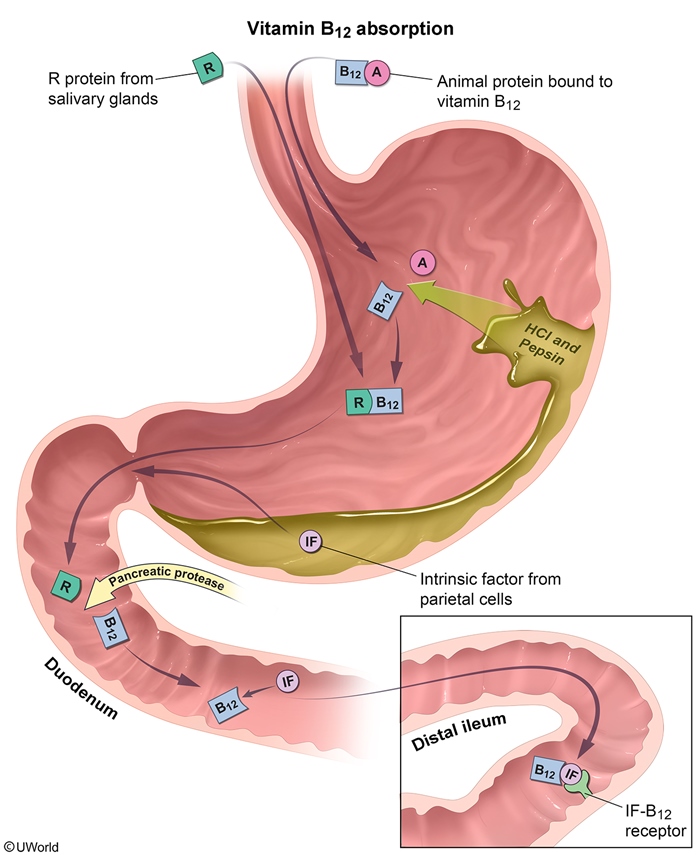
- Pernicious anemia — autoimmune destruction of parietal cells / intrinsic factor (IF). Most common cause of B12 deficiency in adults. Refer to the Atrophic Gastritis: H. pylori-Induced vs Autoimmune Gastritis Comparison for the autoimmune vs infectious distinction.
- Strict veganism — B12 is found exclusively in animal products; body stores last 3–5 years, so deficiency develops slowly (months to years)
- Terminal ileal disease — Crohn disease, ileal resection → B12 is absorbed exclusively in the terminal ileum (requires IF binding). See the Nutrient Deficiencies Associated with Malabsorption for the full malabsorption pattern.
Other notable causes: metformin (long-term use impairs ileal absorption), Diphyllobothrium latum (fish tapeworm consumes luminal B12), gastrectomy/gastric bypass (loss of IF-producing parietal cells).
Folate deficiency — top causes
- Alcoholism — poor dietary intake + impaired jejunal absorption + increased urinary excretion. Most common cause. Folate stores last only 3–4 months, so deficiency develops within weeks to months
- Pregnancy / chronic hemolysis — increased demand from rapid cell turnover. Folate deficiency in early pregnancy → neural tube defects (spina bifida, anencephaly) — occurs in the first 4 weeks, often before pregnancy is recognized
- Drug-induced (folate antagonists) — impair the folate cycle at various steps
| Drugs Causing Folate Deficiency — "Mary, Take Phen-Sulfa Pills" | |
| • Methotrexate (DHFR inhibitor) • Trimethoprim (DHFR inhibitor) • Phenytoin (impairs absorption) • Sulfasalazine (impairs absorption) • Pyrimethamine / Pills (OCPs) |
جملة تذكرية |
See the Folate Antagonists: Mechanisms, Drugs, and Therapeutic Applications for the full drug class breakdown and DHFR inhibition mechanisms.
Absorption site — the clinical clue
- B12 → terminal ileum (requires intrinsic factor). Disease of the terminal ileum = think B12 deficiency
- Folate → jejunum. Disease of the jejunum (celiac, tropical sprue) = think folate deficiency first
Clinical Presentation & Diagnostic Approach
Shared features (B12 and folate)
- Anemia symptoms — fatigue, weakness, pallor, exertional dyspnea
- Mild jaundice (ineffective erythropoiesis → ↑ indirect bilirubin, ↑ LDH)
- Glossitis — smooth, beefy-red tongue; angular cheilitis, oral ulcers
- Anorexia, diarrhea, weight loss (GI epithelial turnover affected)
Neurologic findings — B12 ONLY
May develop before or independent of anemia. Often irreversible if treatment is delayed > 6 months.
- Peripheral neuropathy — symmetric numbness/tingling of feet → hands (earliest symptom)
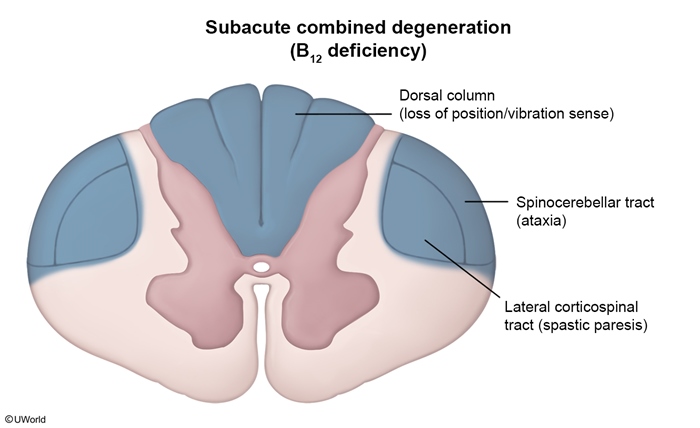
- Subacute combined degeneration:
- Dorsal columns → ↓ vibration, ↓ proprioception, + Romberg sign, sensory ataxia
- Lateral corticospinal tracts → spastic paresis, hyperreflexia, + Babinski
- Spinocerebellar tracts → ataxia
- Cognitive/psychiatric — memory loss, dementia, depression, psychosis ("megaloblastic madness")
| Pernicious Anemia — Exam Vignette | |
| Pernicious anemia is the most common cause of B12 deficiency in adults. Classic stem: • Older patient (50–60s), often Northern European descent • Associated autoimmune diseases: vitiligo, type 1 DM, Hashimoto, Addison • Anti-intrinsic factor antibodies (most specific) or anti-parietal cell antibodies (most sensitive) • Atrophic gastritis of the body/fundus → ↑ gastrin, achlorhydria • ↑ Risk of gastric adenocarcinoma and gastric carcinoid |
تذكر |
Diagnostic approach
Step 1 — CBC + peripheral smear:
- ↑ MCV (> 100 fL; often > 110 in megaloblastic causes)
- Pancytopenia may be present in severe cases (all marrow lineages affected)
- Smear: macro-ovalocytes + hypersegmented neutrophils (≥ 5 lobes) — the earliest and most specific finding
- Low reticulocyte count (distinguishes from hemolysis/hemorrhage)
Step 2 — Confirm and differentiate the deficiency:
- Check serum B12 and serum/RBC folate
- If borderline or equivocal → check MMA and homocysteine:
- ↑ MMA + ↑ homocysteine → B12 deficiency
- Normal MMA + ↑ homocysteine → folate deficiency
| Differentiate B12 vs Folate — "M for B12" | |
| • MMA ↑ = B12 deficiency (Normal in folate) • Myelin damage = B12 only • Months-to-years to deplete stores = B12 (folate depletes in weeks) |
جملة تذكرية |
| Master Comparison: Vitamin B12 vs Folate Deficiency | ||
|---|---|---|
| Feature | B12 (Cobalamin) | Folate (B9) |
| Body stores | 3–5 years (slow depletion) | 3–4 months (rapid depletion) |
| Main dietary sources | Animal products only | Green leafy vegetables, legumes |
| Absorption site | Terminal ileum (requires intrinsic factor) | Jejunum |
| Top causes | Pernicious anemia, veganism, terminal ileal disease (Crohn) | Alcoholism, pregnancy/hemolysis, drugs (MTX, phenytoin) |
| Neurologic symptoms | YES — subacute combined degeneration, peripheral neuropathy, dementia | NO |
| Serum B12 | ↓ (< 200 pg/mL) | Normal |
| Serum / RBC folate | Normal (or falsely ↑) | ↓ |
| Methylmalonic acid (MMA) | ↑↑ — KEY discriminator | Normal |
| Homocysteine | ↑ | ↑ |
| Anti-IF antibodies | Positive in pernicious anemia | Negative |
| Neural tube defect risk | No | Yes — if deficient in pregnancy |
Step 3 — Determine etiology of B12 deficiency:
- Anti-intrinsic factor antibodies — highly specific for pernicious anemia (test of choice)
- Anti-parietal cell antibodies — sensitive but less specific
- Serum gastrin — elevated in pernicious anemia (no acid feedback → hypergastrinemia)
- Endoscopy — if atrophic gastritis or malignancy suspected
Key differential — megaloblastic vs non-megaloblastic macrocytosis
Not every MCV > 100 is megaloblastic. The presence or absence of hypersegmented neutrophils splits the differential:
- Megaloblastic (hypersegmented neutrophils PRESENT): B12 deficiency, folate deficiency, drug-induced (methotrexate, hydroxyurea, 5-FU, AZT)
- Non-megaloblastic (NO hypersegmented neutrophils): alcoholism (direct marrow toxicity), liver disease, hypothyroidism, reticulocytosis, MDS
See the Common Causes of Macrocytic Anemia (MCV >100 μm³) for the complete differential breakdown.
Management & Complications
B12 replacement
- Pernicious anemia / malabsorption → IM cyanocobalamin (or hydroxocobalamin):
- 1000 μg IM daily × 1 week → weekly × 4 weeks → monthly for life
- Dietary deficiency / mild cases → oral B12 1000–2000 μg/day (effective even in pernicious anemia — ~1% is absorbed passively, independent of IF)
- Treat the underlying cause: stop offending medications (PPIs, metformin), manage Crohn disease
Folate replacement
- Oral folic acid 1–5 mg/day for 1–4 months
- Pregnancy prophylaxis: 400 μg/day for all women of reproductive age; 4 mg/day if history of a prior NTD child
- Treat/remove the cause: stop alcohol, change medications, treat celiac disease
| Never Give Folate Alone | |
| NEVER give folate alone if B12 deficiency has not been excluded. Folate corrects the anemia (bypasses the methyl-trap) but does NOT fix the neurologic damage → neuropathy progresses silently and may become irreversible. Rule: Always check B12 first, or empirically give both until B12 is excluded. |
تذكر |
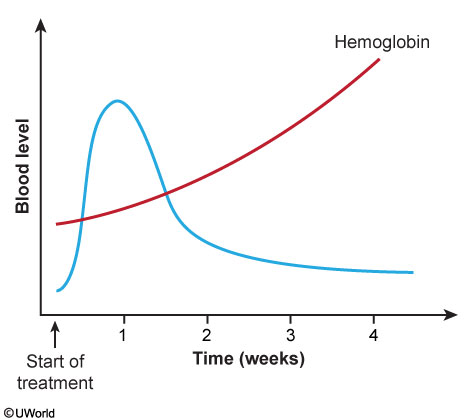
Treatment response — expected timeline
- Day 2–3: subjective improvement; ↓ MMA and homocysteine
- Day 5–7: reticulocyte peak — the earliest objective marker that treatment is working
- 6–8 weeks: hemoglobin normalizes
- Neurologic recovery: weeks to months; may be incomplete if damage persisted > 6 months
- ⚠ Watch for hypokalemia during rapid reticulocyte response — newly forming cells consume K⁺ → risk of arrhythmia in elderly patients
Complications of untreated deficiency
- Untreated B12:
- Permanent neurologic deficits — subacute combined degeneration, dementia, optic atrophy (the most feared complication)
- Severe anemia → high-output heart failure
- Pernicious anemia → ↑ risk of gastric adenocarcinoma and gastric carcinoid (chronic atrophic gastritis → hypergastrinemia → ECL cell hyperplasia)
- Untreated folate in pregnancy: neural tube defects (spina bifida, anencephaly) — occurs in the first 4 weeks, often before pregnancy is recognized
- Both: ↑ homocysteine → ↑ risk of atherosclerosis, thrombosis, MI, stroke
Special situations
- Methotrexate toxicity → rescue with folinic acid (leucovorin) 10–25 mg IV/PO every 6 hours, NOT folic acid (MTX blocks DHFR; leucovorin bypasses the blocked enzyme)
- Nitrous oxide exposure → irreversibly oxidizes B12 → can precipitate acute megaloblastic crisis in patients with borderline B12 stores
- Trimethoprim-induced → can be reversed with leucovorin if clinically significant
Key Clinical Vignettes – نقاط مهمة للامتحانات
The following scenarios reflect the most frequently tested patterns on SMLE, USMLE, and JMC exams.
Vignette 1 — B12 deficiency with neurologic findings
Stem: A 70-year-old woman presents with fatigue, exertional dyspnea, and frequent falls. Exam shows symmetrically decreased vibratory sensation in the lower extremities. Hgb 7.8 g/dL; peripheral smear shows hypersegmented neutrophils.
- Diagnosis: Megaloblastic anemia due to B12 deficiency — neurologic symptoms (↓ vibration = dorsal column) clinch B12 over folate
- Treatment: IM cyanocobalamin 1000 μg — not folate alone
- Teaching point: Neurologic findings + megaloblastic anemia = B12 until proven otherwise
Vignette 2 — Folate deficiency in an alcoholic
Stem: A 55-year-old man with heavy alcohol use (3–4 drinks/day for years) presents with fatigue. Labs show MCV 110 fL, hepatomegaly from fatty liver.
- Diagnosis: Folate deficiency — alcohol impairs folate absorption and increases excretion; limited body stores deplete within weeks
- Key distinction: Alcoholism can also cause non-megaloblastic macrocytosis (direct marrow toxicity) — check smear for hypersegmented neutrophils to confirm megaloblastic cause
Vignette 3 — Folate masking B12 neuropathy
Stem: A 54-year-old man with megaloblastic anemia is started on folic acid. At 4-week follow-up, Hgb has improved (9.1 g/dL) but he reports new tingling in his toes.
- Diagnosis: Undiagnosed B12 deficiency masked by folate therapy
- Mechanism: Folate corrected the anemia (bypassed the methyl-trap) but B12-dependent myelination was never addressed → subacute combined degeneration progresses
- Teaching point: This is the reason you must always exclude B12 deficiency before giving folate alone
Vignette 4 — Mechanism question
Stem: A patient with macrocytic anemia and hypersegmented neutrophils. "What is the underlying pathophysiology?"
- Answer: Impaired DNA synthesis — B12/folate deficiency disrupts thymidine (dTMP) production → delayed nuclear division relative to cytoplasmic maturation → nuclear–cytoplasmic asynchrony
| Nitrous Oxide Trap | |
| A patient with borderline B12 stores (e.g., vegan, elderly, post-gastric bypass) who undergoes general anesthesia with nitrous oxide (N₂O) can develop acute megaloblastic anemia and neurologic deterioration. N₂O irreversibly oxidizes the cobalt in B12 → inactivates methionine synthase → precipitates sudden B12 crisis. This is a classic boards question — always screen B12 status before N₂O exposure in at-risk patients. |
تذكر |
Rapid-fire exam pearls
- Hypersegmented neutrophils (≥ 5 lobes) = earliest and most specific morphologic sign of megaloblastic anemia
- ↑ MMA = B12 deficiency; normal MMA = folate deficiency — this is the single best lab to differentiate the two
- Reticulocyte peak at day 5–7 = confirms treatment response
- Hypokalemia during treatment — newly forming cells consume K⁺; monitor in elderly
- Pernicious anemia → anti-IF antibodies (specific), ↑ gastrin, ↑ risk of gastric carcinoma/carcinoid
- Folate 400 μg/day for all women of reproductive age; 4 mg/day if prior NTD
- Leucovorin (folinic acid) rescues methotrexate toxicity — bypasses DHFR block; folic acid does not
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.