شرح المدرسين

Introduction
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
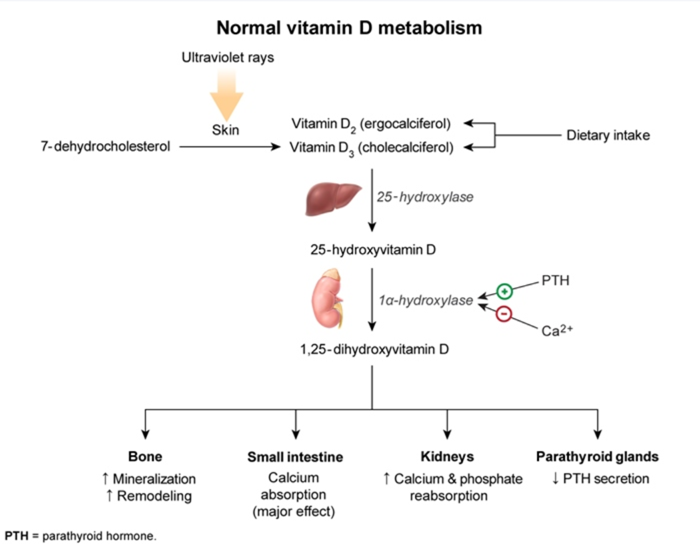
Vitamin D Metabolism
- Synthesis: Vitamin D is synthesized in the skin (cholecalciferol, Vitamin D3) from 7-dehydrocholesterol upon exposure to UVB radiation.
- Hydroxylation:
- First hydroxylation occurs in the liver, converting Vitamin D3 to 25-hydroxyvitamin D [25(OH)D], the major circulating form.
- Second hydroxylation occurs in the kidney, converting 25(OH)D to its active form, 1,25-dihydroxyvitamin D [1,25(OH)2D], or calcitriol.
- Function:
- Increases calcium and phosphate absorption from the gut
- Increases calcium and phosphate reabsorption in the distal convoluted tubules of the kidney
- Modulates bone mineralization.
- Regulation: If the Ca+2 level is low, active vitamin D increases bone resorption of calcium (moving calcium from bone and into the circulation).
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Vitamin D Daily Supplementation
- Vitamin D levels are very low in breast milk, so exclusively breastfed infants need supplementation.
- For older children with adequate exposure to sunlight, vitamin D supplementation is usually not necessary.
- The recommended dose of vitamin D for children is 400 IU per day.
- This recommended dosage begins within the first few days after birth and continues throughout adolescence
| Vitamin D Daily Supplementation | |
|---|---|
| Population | Recommended Daily Dose |
| Infants (0–12 months) | 400 IU/day |
| Children (1–18 years) | 600–1,000 IU/day |
| Adults (19–70 years) | 600–2,000 IU/day |
| Elderly (> 70 years) | 800–2,000 IU/day |
| Pregnant & lactating women | 600–2,000 IU/day |
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
Vitamin D Deficiency
Introduction
- Rickets: A pediatric bone disorder caused by defective mineralization of the growth plate and newly formed bone, leading to soft and weakened bones.
- Primary Rickets: Occurs due to deficiencies in vitamin D, calcium, or phosphate, which impair osteoid mineralization.
- Secondary Rickets: Caused by genetic mutations affecting vitamin D metabolism or phosphate regulation, chronic kidney disease, or liver disorders.
- In adults, the equivalent condition is called osteomalacia, where mature bone mineralization is impaired.
- It’s a worldwide problem, affecting 30-60% of the population in all tested countries.
Causes of Vitamin D Deficiency
- Inadequate sun exposure: Limited UVB exposure, use of sunscreen, living in higher latitudes.
- Dietary insufficiency: Low intake of vitamin D-rich foods such as fish and fortified milk.
- Chronic intestinal inflammation: Seen in conditions like untreated celiac disease and Crohn's disease.
- Renal or hepatic dysfunction: These impair the conversion of vitamin D into its active forms.
- Obesity: Vitamin D gets sequestered in adipose (fat) tissue.
- Medications: Certain drugs like glucocorticoids and anticonvulsants can reduce vitamin D levels.
Types of Rickets
- Nutritional Rickets: Caused by deficiencies in vitamin D, calcium, or phosphate.
- Vitamin D-Dependent Rickets:
- Type 1: Autosomal recessive disorder caused by 1-alpha-hydroxylase deficiency, leading to impaired conversion of 25(OH)D to 1,25(OH)D (calcitriol). Patients require vitamin D supplementation.
- Type 2: Caused by mutations in the vitamin D receptor (VDR), leading to tissue insensitivity to calcitriol.
- Hypophosphatemic Rickets: An X-linked disorder marked by impaired renal phosphate retention, resulting in low serum phosphate and impaired bone mineralization.
Clinical Manifestations
- The most common presentation in infants and children with rickets is asymptomatic, meaning many cases are detected incidentally.
- Diagnosis is often made during physical examination or routine lab screening.
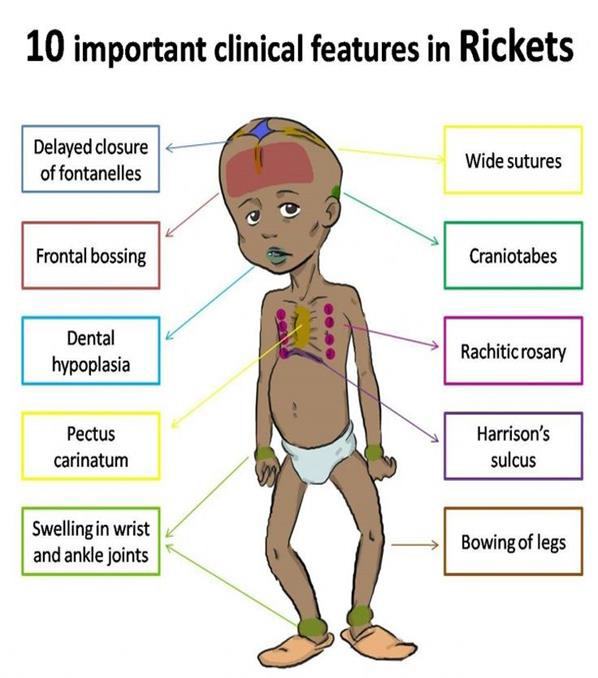
- Other common manifestations of rickets include:
- Bone-related symptoms
- Bone pain or tenderness (arms, legs, spine, pelvis).
- Skeletal deformities
- Bowlegs (genu varus).
- Pigeon chest (forward projection of the breastbone).
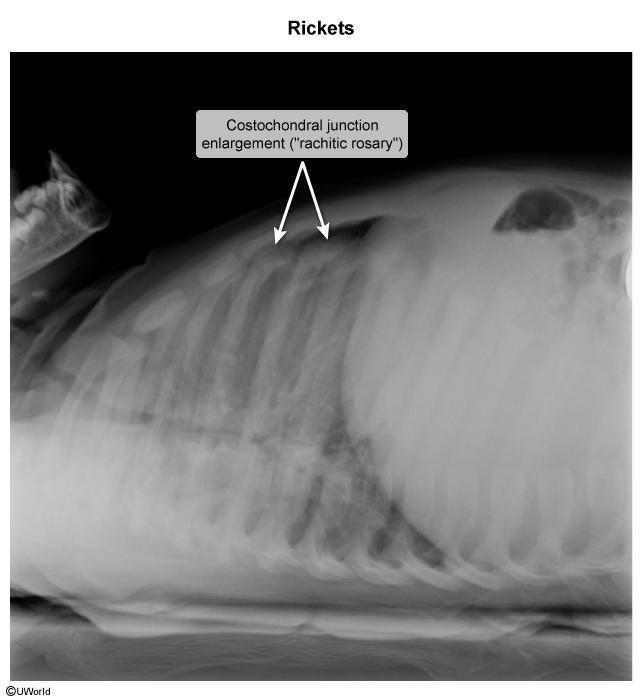
- Rachitic rosary (enlargement of the costochondral joints of the ribs).
- Craniotabes (soft skull bones with a "pingpong ball" feel).
- Asymmetrical or oddly shaped skull.
- Harrison’s sulci (horizontal grooves at the lower ribs).
- Spine deformities such as scoliosis and kyphosis.
- Pelvic deformities.
- Other manifestations
- Increased risk of bone fractures.
- Dental abnormalities:
- Delayed eruption of teeth.
- Defective enamel with pits or holes.
- Increased dental cavities.
- Muscle issues: Cramps and muscle weakness.
- Growth delays and short stature.
- Bone-related symptoms
Diagnosis
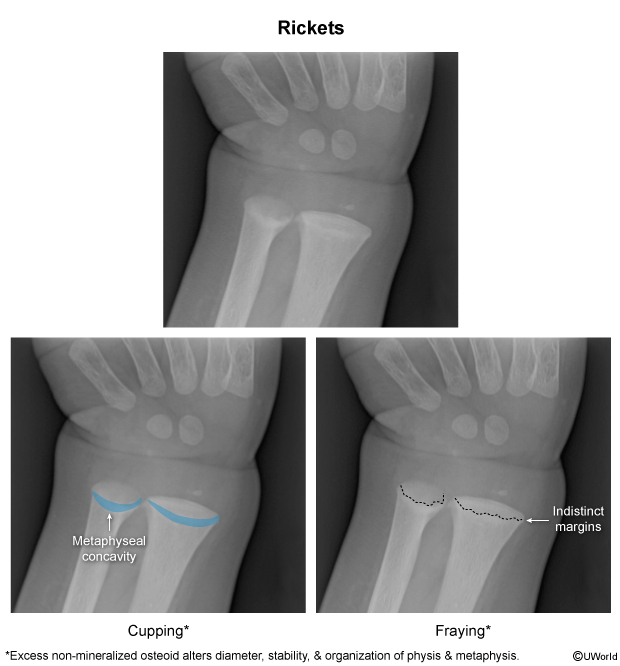
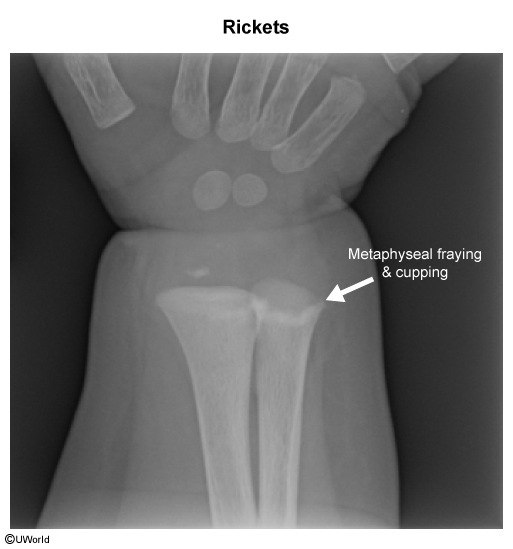
- Rickets is usually diagnosed through radiographic (X-ray) examination of the long bones.
- Findings may include:
- Osteopenic bone shafts (low bone density).
- Widened growth plates.
- Frayed and cupped metaphyseal ends (irregular and blurred bone ends).
- After starting vitamin D therapy, the long bone ends often appear brighter on X-ray, indicating healing.
| Types of Rickets | |||||||
|---|---|---|---|---|---|---|---|
| Type of Rickets | Mode of Inheritance | Calcium | Phosphate | 25(OH) Vitamin D | 1,25(OH) Vitamin D | Alkaline Phosphatase | PTH |
| Nutritional Rickets | None (environmental) | Low/Normal | Low/Normal | Low | Low | High | High |
| Vitamin D-Dependent Type 1 | Autosomal Recessive | Low | Low | Normal | Low | High | High |
| Vitamin D-Dependent Type 2 | Autosomal Recessive | Low | Low | Normal | High | High | High |
| X-Linked Hypophosphatemic Rickets (XLH) | X-Linked Dominant | Normal | Low | Normal | Normal | High | Normal |
| Autosomal Dominant Hypophosphatemic Rickets (ADHR) | Autosomal Dominant | Normal | Low | Normal | Normal | High | Normal |
Treatment of Vitamin D Deficiency and Rickets
- Vitamin D Supplementation:
- Mild deficiency: 600–2,000 IU/day of vitamin D.
- Severe deficiency: 50,000 IU/week for 6–8 weeks followed by maintenance dosing.
- For rickets: High-dose oral vitamin D (up to 2,000–6,000 IU/day) or calcitriol for genetic forms.
- Calcium supplementation: Often required in cases of severe deficiency or rickets.
- Treatment of Vitamin D-Dependent Rickets:
- Type 1: Calcitriol supplementation.
- Type 2: High-dose calcitriol and calcium, with close monitoring of biochemical response.
سجل دخولك لإضافة ملاحظات خاصة لكل قسم
· اشترك الآن
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.
فيديوهات الشرح
بطاقات تفاعلية
أسئلة ممارسة
اشترك الآن