Summary
Female infertility, defined as failure to conceive after 12 months of unprotected intercourse (6 months if ≥36 years), is most often due to ovulatory dysfunction, tubal disease, endometriosis, or uterine abnormalities. Evaluation involves confirming ovulation, assessing ovarian reserve, and investigating tubal and uterine factors, while management ranges from lifestyle modification and ovulation induction to surgical correction and assisted reproductive techniques such as IUI, IVF, or ICSI.
Causes
1. Disorders of Ovulation
Ovulatory dysfunction is the most common cause of female infertility and has been classified by the World Health Organization into three groups:
-
Group I: Hypothalamic–pituitary failure (≈10%)
-
Hypothalamic amenorrhea (low body weight, excessive exercise, eating disorders)
-
Hypogonadotropic hypogonadism (e.g., Kallmann syndrome)
-
Group II: Hypothalamic–pituitary–ovarian dysfunction (≈85%)
-
Predominantly polycystic ovary syndrome (PCOS)
-
Associated with insulin resistance, obesity, and metabolic syndrome
-
Group III: Ovarian failure (≈4–5%)
-
Hypergonadotropic hypogonadism (premature ovarian insufficiency)
-
May result from genetic causes, autoimmune disease, or prior chemotherapy/radiotherapy
2. Tubal and Peritoneal Causes
-
Pelvic inflammatory disease (PID) leading to tubal scarring or obstruction
-
Endometriosis causing adhesions and distortion of pelvic anatomy
-
Previous sterilization procedures or pelvic surgery
-
Hydrosalpinx impairing implantation
3. Uterine Causes
-
Fibroids (leiomyomas), especially submucosal
-
Endometrial polyps
-
Congenital uterine anomalies (septate, bicornuate uterus, Mayer-Rokitansky-Küster-Hauser syndrome)
-
Asherman’s syndrome (intrauterine adhesions)
4. Cervical Causes
-
Insufficient cervical mucus production
-
Cervical trauma (e.g., after conization, cryotherapy)
-
Congenital cervical anomalies
-
Immune-mediated factors (e.g., antisperm antibodies)
-
In utero exposure to diethylstilbestrol (DES)
5. Other Causes
-
Unexplained infertility (10–20% of cases)
-
Genetic abnormalities
-
Systemic and immune disorders (e.g., thyroid disease, systemic lupus erythematosus)
-
Medications (chemotherapy, cytotoxic agents)
-
Lifestyle factors: obesity, underweight, smoking, excessive alcohol, high stress
Initial Evaluation in Primary Care
Investigations are recommended after 12 months of attempted conception (6 months if age ≥36 years or if risk factors are present).
-
Ovulation assessment: Mid-luteal serum progesterone (day 21 in a 28-day cycle; >3 ng/mL indicates ovulation)
-
Chlamydia screening
-
Rubella immunity testing
-
Additional tests when indicated:
-
Serum gonadotropins (FSH, LH) in women with irregular cycles
-
Thyroid function tests and prolactin if suggestive symptoms are present
-
Anti-Müllerian hormone (AMH) and antral follicle count for ovarian reserve assessment
Referral to secondary care is warranted earlier if there is a history of amenorrhea, oligomenorrhea, previous pelvic surgery or PID, abnormal pelvic examination, previous cancer treatment, or maternal age ≥36 years.
Secondary Care Investigations
-
Assessment of tubal patency:
-
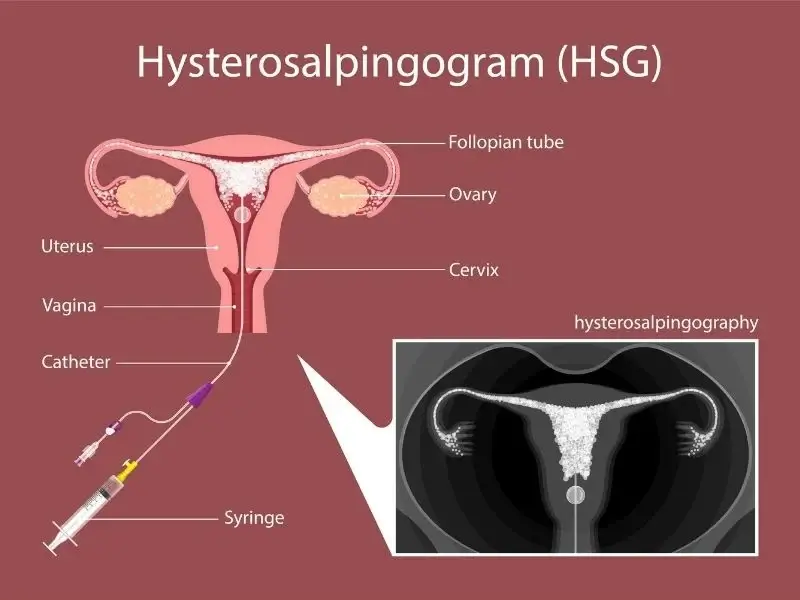
Hysterosalpingography (HSG) or hysterosalpingo-contrast sonography in women without comorbidities
-
Diagnostic laparoscopy with chromopertubation in women with endometriosis, PID, or prior pelvic surgery
-
Imaging: Transvaginal ultrasound for uterine, cervical, or adnexal pathology
- Hysteroscopy: For intrauterine abnormalities such as fibroids, polyps, or adhesions
| Keep in mind: | |
| A stepwise diagnostic approach includes confirmation of ovulation, assessment of tubal patency, and evaluation for uterine pathology. | ملاحظة |
Management of Female Infertility
1. Lifestyle Modification
-
Achieve and maintain a healthy body weight (BMI 19–25 kg/m²)
-
Smoking cessation and alcohol reduction
-
Stress management and counseling support
2. Medical Management
-
Ovulation induction:
-
First-line: Letrozole (off-label, preferred in PCOS) or clomiphene citrate
-
If resistant: Gonadotropins (FSH, LH, hCG) or laparoscopic ovarian drilling
-
Hypothalamic amenorrhea: Pulsatile GnRH
-
Hyperprolactinemia: Dopamine agonists (e.g., bromocriptine, cabergoline)
-
Endocrine disorders: Treat underlying hypothyroidism, hyperprolactinemia, or insulin resistance
3. Surgical Management
-
Tuboplasty or salpingectomy in tubal disease
-
Laparoscopic excision/ablation of endometriosis
-
Hysteroscopic removal of intrauterine adhesions, fibroids, or polyps
4. Medically Assisted Reproduction
-
Intrauterine insemination (IUI): Placement of washed sperm directly into the uterine cavity at ovulation
-
In vitro fertilization (IVF): Ovarian stimulation, oocyte retrieval, extracorporeal fertilization, embryo transfer
-
Intracytoplasmic sperm injection (ICSI): For severe male or fertilization-related infertility
-
Use of donor gametes or surrogacy when indicated
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.