شرح المدرسين

Summary
Hematology is the study of blood and the organs that make it (bone marrow, spleen, lymph nodes, thymus). Blood has two parts:
- Plasma (55%) – water, proteins (albumin, clotting factors, immunoglobulins), electrolytes.
- Cells (45%) – red blood cells (RBCs), white blood cells (WBCs), and platelets.
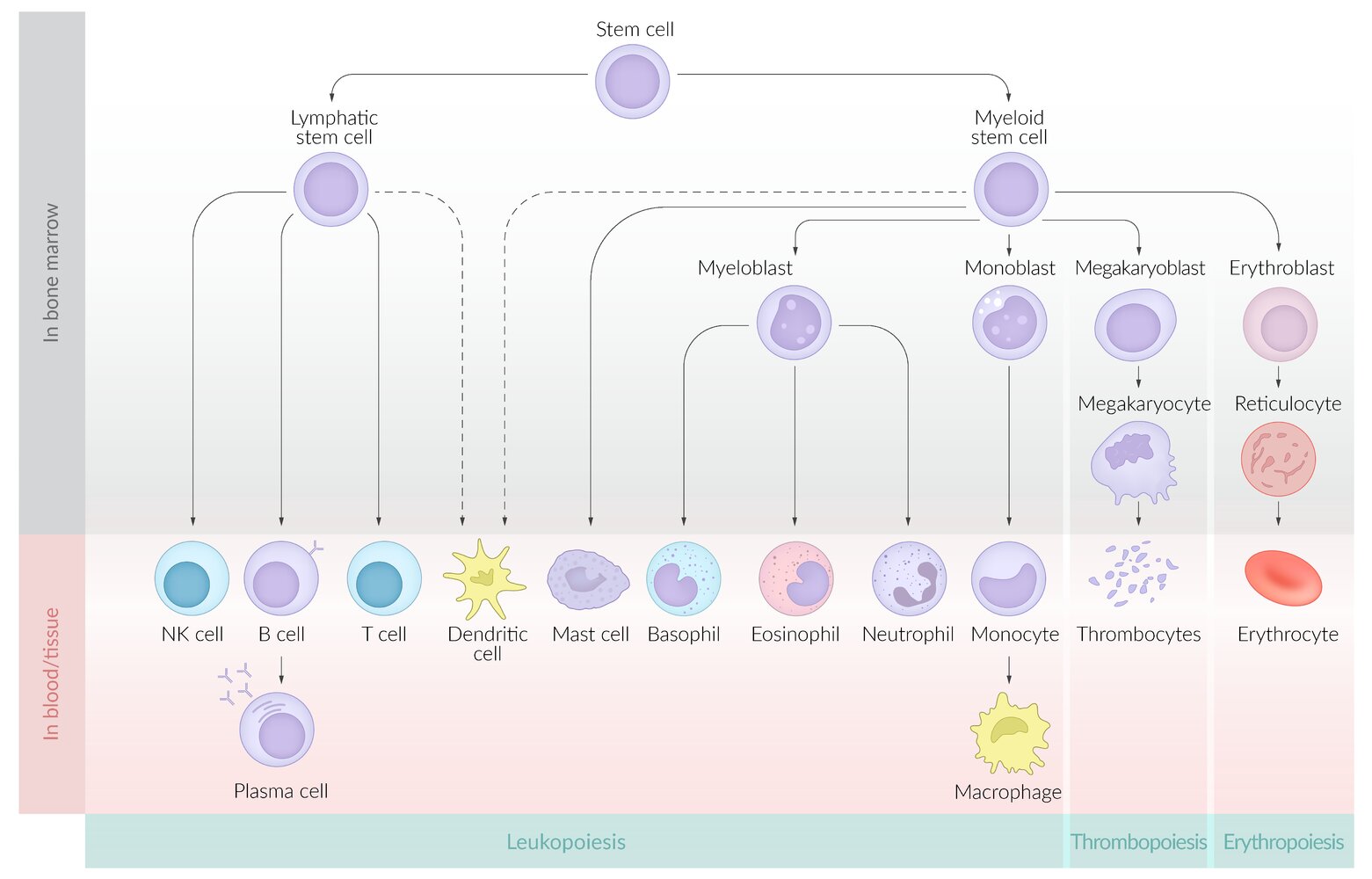
All blood cells come from a single hematopoietic stem cell (HSC) in the bone marrow. They split into two main lines:
- Myeloid line → RBCs, platelets, granulocytes (neutrophil, eosinophil, basophil), monocytes.
- Lymphoid line → B cells, T cells, NK cells.
This first lesson gives you the framework you need before studying anemias, leukemias, bleeding disorders, and transfusion medicine. Focus on three big ideas:
- How blood cells are made (hematopoiesis).
- How blood stops bleeding (hemostasis).
- How to read a basic CBC and peripheral smear.
Blood composition
When you spin a tube of blood in a centrifuge, it separates into three layers:
- Plasma (top, ~55%): yellow fluid; contains albumin, globulins, fibrinogen, clotting factors, hormones, electrolytes.
- Buffy coat (thin middle layer, <1%): WBCs and platelets.
- RBCs (bottom, ~45%): this volume = the hematocrit (Hct).
Serum = plasma after clotting (no fibrinogen, no clotting factors). This is what most chemistry tests use.
Key cell counts (adult)
- RBCs: 4.5–5.5 million/μL
- Hemoglobin (Hgb): M 13.5–17.5 g/dL · F 12–16 g/dL
- Hematocrit: M ~41–53% · F ~36–46%
- WBCs: 4,000–11,000/μL
- Platelets: 150,000–400,000/μL
Lifespan: RBC ~120 days · platelet ~7–10 days · neutrophil hours to days · lymphocyte days to years.
Hematopoiesis
Hematopoiesis = the process of making blood cells. It happens in different sites depending on age:
- 0–2 months fetal life: yolk sac
- 2–7 months: liver and spleen
- From 7 months onward: bone marrow
- Adult: bone marrow of axial skeleton (vertebrae, sternum, ribs, pelvis, proximal femur/humerus)
All cells start from one pluripotent hematopoietic stem cell (HSC), which divides into:
- Common myeloid progenitor → RBCs, platelets, granulocytes (neutrophil, eosinophil, basophil), monocytes/macrophages.
- Common lymphoid progenitor → B cells, T cells, NK cells.
Key cytokines (who tells the cells to grow?)
Cytokines are chemical messengers that act as master directors, telling bone marrow cells exactly when and how to grow and differentiate into mature blood cells.
السيتوكينات (Cytokines): هي الرسل الكيميائية والمُوجّه الأساسي الذي يخبر خلايا النخاع العظمي كيف ومتى تنمو وتتمايز لتنتج خلايا الدم المختلفة.
| Key Cytokines in Hematopoiesis | |
|---|---|
| Cytokine | Primary Function & Clinical Link |
| EPO (Erythropoietin) | From the kidney → stimulates RBC production. |
| TPO (Thrombopoietin) | From the liver → stimulates platelet production. |
| G-CSF | Stimulates neutrophils (given post-chemotherapy). |
| IL-3 | "The bone marrow IL" → supports all cell lines (acts at the stem cell level). |
| IL-5 | Stimulates eosinophils. |
💡 Clinical Pearls (High-Yield Exam Points)
-
🔴 Renal Failure → ↓ EPO → Normocytic Anemia (A very common exam scenario!)
-
🟡 Liver Failure → ↓ TPO → Thrombocytopenia (low platelet count).
-
🟢 Post-Chemotherapy → Give G-CSF to prevent life-threatening neutropenia.
-
🔵 IL-3 → The only one that supports all lines because it works directly at the stem cell level itself.
Red blood cells and hemoglobin
RBCs are biconcave discs, no nucleus, no mitochondria. They carry oxygen using hemoglobin (Hb).
Hemoglobin structure
- 4 globin chains + 4 heme groups (each holds 1 Fe²⁺ → binds 1 O₂)
- HbA (adult, >95%) = 2α + 2β
- HbA2 (~2%) = 2α + 2δ — ↑ in β-thalassemia
- HbF (fetal, <1% in adult) = 2α + 2γ — higher O₂ affinity
Oxygen-dissociation curve
The Hb curve is sigmoid (cooperative binding); myoglobin is hyperbolic. P50 of Hb ≈ 26 mm Hg.
Think of it as one simple question: is hemoglobin giving oxygen to the tissues, or keeping it?
- Right shift = Hb gives O₂ away (lets go) → happens when tissues need more oxygen, like an exercising muscle: ↑ CO₂, ↑ H⁺ (low pH), ↑ temperature, ↑ 2,3-BPG. P50 goes up.
- Left shift = Hb keeps O₂ (holds on) → the exact opposite (low CO₂, high pH, cold, low 2,3-BPG), plus HbF, CO poisoning, and methemoglobin. P50 goes down.
| الفكرة ببساطة – Right vs Left shift | |
Right shift (انزياح لليمين) = الهيموغلوبين "يفلت" الأكسجين للأنسجة. يحدث في الظروف التي تحتاج فيها الأنسجة أكسجين أكثر، مثل العضلة أثناء التمرين: حرارة عالية، حموضة (pH منخفض)، CO₂ مرتفع، و2,3-BPG مرتفع. Left shift (انزياح لليسار) = الهيموغلوبين "يمسك" الأكسجين ولا يطلقه بسهولة. هو عكس اليمين تماماً (برودة، pH مرتفع، CO₂ منخفض، 2,3-BPG منخفض)، بالإضافة إلى HbF وتسمم CO والميتهيموغلوبين. حيلة سريعة: اليمين = إطلاق (Release) للأنسجة → P50 يرتفع. اليسار = احتباس (Load/hold) → P50 ينخفض. |
ملاحظة |
Oxygen-dissociation curve (click)
Erythropoiesis in 1 line
Low O₂ → kidney makes EPO → bone marrow makes RBCs (proerythroblast → erythroblast → normoblast → reticulocyte → mature RBC).
Reticulocyte count tells you if the marrow is responding: high = marrow working (e.g., hemolysis, bleeding); low = marrow failure or deficiency (Fe, B12, folate).
Erythropoiesis stages (click)
White blood cells
WBCs are the immune cells. Normal total = 4,000–11,000/μL.
Differential (typical adult)
- Neutrophils 40–70% – first responders to bacterial infection. Multi-lobed nucleus.
- Lymphocytes 20–40% – B, T, NK cells; viral infections, chronic inflammation.
- Monocytes 2–10% – mature into tissue macrophages.
- Eosinophils 1–6% – parasites, allergy.
- Basophils <1% – allergy, releases histamine.
Patterns to recognize
- Neutrophilia + left shift (more bands/immature forms) → acute bacterial infection.
- Lymphocytosis + atypical lymphocytes → viral (think EBV, CMV).
- Eosinophilia (NAACP): Neoplasia, Allergy/Asthma, Adrenal insufficiency, Collagen vascular disease, Parasites.
- Neutropenia (<1,500/μL) → infection risk; <500 = severe → febrile neutropenia is an emergency.
Memorize the differential percentages with the mnemonic "Never Let Monkeys Eat Bananas" in order of frequency: Neutrophil > Lymphocyte > Monocyte > Eosinophil > Basophil.
Hemostasis – primary and secondary
When a vessel is injured, the body stops the bleeding in two coordinated steps.
1. Primary hemostasis (platelet plug)
Happens in seconds. Involves platelets + von Willebrand factor (vWF).
- Vasoconstriction – endothelial injury → reflex constriction.
- Adhesion – platelets bind exposed collagen via vWF using GPIb receptor.
- Activation – platelets release ADP, TXA2 → recruit more platelets.
- Aggregation – platelets stick to each other via GPIIb/IIIa and fibrinogen.
Defects → mucocutaneous bleeding (gums, nose, petechiae, easy bruising). Examples: ITP, vWD, Bernard-Soulier (no GPIb), Glanzmann (no GPIIb/IIIa).
Primary hemostasis diagram (click)2. Secondary hemostasis (coagulation cascade)
Happens over minutes. Activates clotting factors → ends with fibrin stabilizing the platelet plug.
- Extrinsic pathway = tissue factor + VII. Measured by PT/INR. (Warfarin works here.)
- Intrinsic pathway = XII → XI → IX → VIII. Measured by aPTT. (Heparin works here.)
- Common pathway = X → V → II (prothrombin → thrombin) → I (fibrinogen → fibrin) → XIII (cross-links fibrin).
Defects → deep bleeding (hemarthrosis, intramuscular hematoma, delayed bleeding after surgery). Examples: hemophilia A (factor VIII), hemophilia B (IX), vitamin K deficiency (II, VII, IX, X, C, S).
Coagulation cascade (click)Approach to Anemia (MCV-Based)
- Anemia = ↓ hemoglobin (M <13.5 g/dL, F <12 g/dL) or ↓ hematocrit.
- Key symptoms: fatigue, pallor, dyspnea on exertion, tachycardia.
- Additional clues by type: koilonychia & pica (IDA), glossitis (B12/folate), jaundice (hemolysis).
The first step in every anemia workup is the MCV (mean corpuscular volume) — it immediately narrows the differential into three categories: microcytic, normocytic, and macrocytic. Reticulocyte count then subdivides the normocytic group.
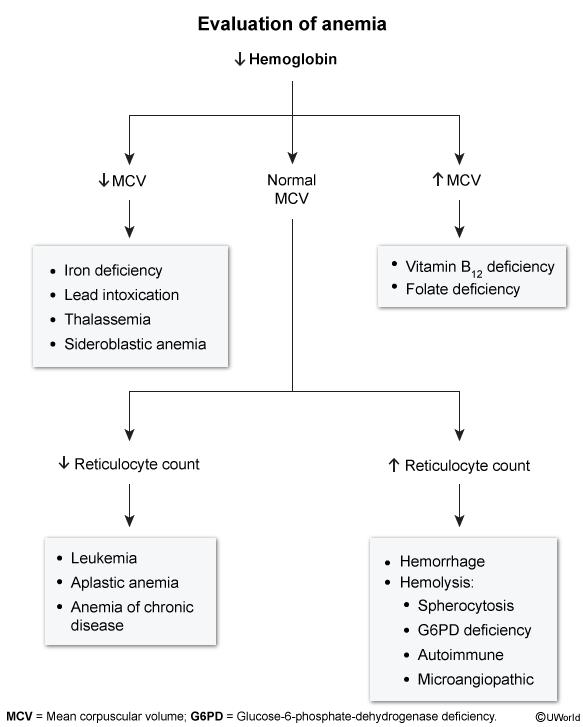
1. Microcytic Anemia (< 80 fL)
Common causes:
- Iron deficiency anemia (IDA) — most common
- Thalassemia
- Anemia of chronic disease (ACD)
- Sideroblastic anemia
- Lead poisoning
| Microcytic Anemia Causes — "TAILS" | |
| T – Thalassemia A – Anemia of chronic disease I – Iron deficiency (most common!) L – Lead poisoning S – Sideroblastic anemia |
جملة تذكرية |
Key lab findings (iron studies):
- IDA: ↓Fe, ↓Ferritin, ↑TIBC, ↓Sat
- Thalassemia: Normal/↑Fe, Normal/↑Ferritin, Normal TIBC
- ACD: ↓Fe, Normal/↑Ferritin, ↓TIBC (hepcidin ↑ → iron trapped in macrophages; ferritin is an acute-phase reactant)
- IDA vs. Thalassemia trap: ferritin is the key discriminator (IDA = ↓ferritin; thalassemia = normal/↑ferritin). RDW is ↑ in IDA (variable cell sizes) but normal in thalassemia (uniformly small cells).
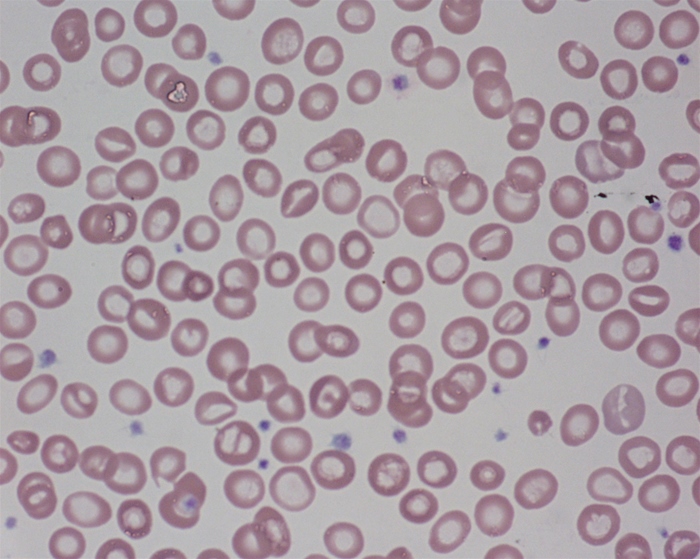
Classic smear findings:
- Hypochromic microcytes with central pallor exceeding ⅓ of the cell diameter
- Pencil cells (elliptocytes) → IDA
- Target cells → thalassemia
- Basophilic stippling → lead poisoning / sideroblastic anemia
2. Normocytic Anemia (80–100 fL)
Common causes:
- Acute blood loss
- Hemolytic anemias
- CKD (↓ EPO)
- Aplastic anemia
- Early IDA / early ACD
Key lab findings — split by reticulocyte count:
- High retic (>2 %): hemolysis or bleed → ↑LDH, ↓haptoglobin, ↑indirect bilirubin. A reticulocyte index >2 % means the marrow is working → think hemolysis or bleeding, NOT marrow failure.
- Low retic: marrow failure → pancytopenia (aplastic anemia), ↓EPO (CKD)
Classic smear findings:
- Schistocytes → microangiopathic hemolytic anemia (MAHA)
- Spherocytes → hereditary spherocytosis / AIHA
- Sickle cells → sickle cell disease
3. Macrocytic Anemia (> 100 fL)
Common causes:
- Megaloblastic: B12 deficiency, folate deficiency
- Non-megaloblastic: liver disease, alcohol use, hypothyroidism, drugs (MTX, hydroxyurea, AZT)
Key lab findings:
- B12 deficiency: ↑MMA + ↑homocysteine; causes subacute combined degeneration (neuro findings)
- Folate deficiency: normal MMA, ↑homocysteine; no neuro findings
- B12 vs. Folate: both raise homocysteine; only B12 deficiency raises methylmalonic acid (MMA) — the most specific discriminator.
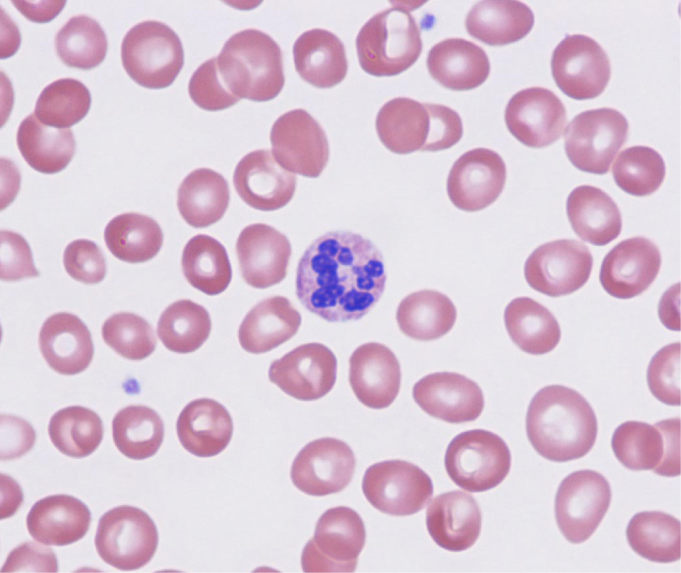
Classic smear findings:
- Megaloblastic: hypersegmented neutrophils (≥5 lobes) — one of the earliest and most specific findings; their presence alone should prompt B12/folate workup. Also macro-ovalocytes.
- Non-megaloblastic: round macrocytes with no hypersegmentation; target cells (liver disease)
| ملاحظة سريرية — فقر الدم | |
|
ملاحظة |
Approach to bleeding disorders
When a patient bleeds abnormally, ask three questions:
- Where is the bleeding? Mucocutaneous (platelet/vWF problem) vs. deep tissue (coagulation factor problem).
- What does the platelet count show? Low → thrombocytopenia; normal → think function defect or coagulation.
- What do PT and aPTT show?
| PT/aPTT interpretation | ||
|---|---|---|
| Pattern | Pathway affected | Think of |
| ↑ PT, normal aPTT | Extrinsic (VII) | Warfarin, early vitamin K deficiency, liver disease |
| Normal PT, ↑ aPTT | Intrinsic (VIII, IX, XI, XII) | Hemophilia A/B, vWD, heparin |
| ↑ PT and ↑ aPTT | Common pathway or multiple | DIC, severe liver disease, vit K def, warfarin overdose |
| Normal PT, normal aPTT, bleeding | Platelet function or vessel | vWD (mild), antiplatelets, factor XIII def, scurvy |
|
Laboratory characteristics of coagulopathies |
|||||
|
Platelet count |
Prothrombin time |
Partial thromboplastin time |
Plasma fibrinogen values |
Peripheral blood smear |
|
|
von Willebrand disease |
Normal |
Normal |
↑ |
Normal |
Normal |
|
Immune thrombocytopenic purpura |
↓ |
Normal |
Normal |
Normal |
Isolated thrombocytopenia |
|
TTP-HUS |
↓ |
Normal |
Normal |
Normal |
RBC fragmentation |
|
Disseminated intravascular coagulation |
↓ |
↑ |
↑ |
↓ |
RBC fragmentation |
| HUS = hemolytic uremic syndrome; RBC = red blood cell; TTP = thrombotic thrombocytopenic purpura. | |||||
Essential lab tests in hematology
Complete Blood Count (CBC)
The starting point for almost every hematology problem. Look at:
- Hgb / Hct – anemia or polycythemia.
- MCV – classifies anemia by size.
- RDW – red cell size variation. ↑ in IDA, mixed deficiency.
- WBC + differential – infection, leukemia screening.
- Platelet count – thrombocytopenia or thrombocytosis.
Peripheral blood smear
Cheap but powerful. Look for abnormal shapes:
- Schistocytes (fragmented) → MAHA: TTP, HUS, DIC.
- Spherocytes → hereditary spherocytosis, warm AIHA.
- Target cells → thalassemia, liver disease, post-splenectomy.
- Sickle cells → sickle cell disease.
- Hypersegmented neutrophils → B12/folate deficiency.
- Howell-Jolly bodies → asplenia/hyposplenism.
- Basophilic stippling → lead poisoning, sideroblastic anemia.
Other key tests
- Reticulocyte count – marrow response.
- Iron studies – Fe, ferritin, TIBC, % saturation.
- LDH, haptoglobin, indirect bilirubin – hemolysis.
- Coombs test (DAT) – autoimmune hemolysis.
- PT, aPTT, INR, fibrinogen, D-dimer – coagulation.
- Bone marrow biopsy – when peripheral tests don't give the answer (leukemia, MDS, aplastic anemia, myeloma).
Mnemonics
| Mnemonic – Vitamin K-dependent factors | |
|
"1972" → factors II, VII, IX, X + proteins C and S. Warfarin inhibits all of them. Protein C/S have shorter half-lives → early hypercoagulability (warfarin-induced skin necrosis). |
جملة تذكرية |
| Mnemonic – WBC differential order | |
|
"Never Let Monkeys Eat Bananas" – from most to least common: Neutrophils > Lymphocytes > Monocytes > Eosinophils > Basophils. |
جملة تذكرية |
| Mnemonic – Causes of eosinophilia (NAACP) | |
|
جملة تذكرية |
| Mnemonic – Right shift of O₂ curve (CADET, face Right!) | |
|
CO₂ ↑ · Acid ↑ (low pH) · 2,3-DPG ↑ · Exercise · Temperature ↑ → curve shifts right → Hb releases O₂ to tissues. |
جملة تذكرية |
Key Points for Exams – نقاط مهمة للامتحانات
- All blood cells come from a pluripotent HSC in the bone marrow → myeloid (RBCs, platelets, granulocytes, monocytes) and lymphoid (B, T, NK) lines.
- EPO from kidney drives RBC production; TPO from liver drives platelets.
- HbA = 2α2β · HbA2 = 2α2δ (↑ in β-thal) · HbF = 2α2γ (higher O₂ affinity).
- Right shift of O₂ curve = release O₂ to tissues (high CO₂, H⁺, 2,3-BPG, temperature).
- Primary hemostasis = platelet + vWF → mucocutaneous bleeding when broken.
- Secondary hemostasis = coagulation factors → deep bleeding (hemarthrosis) when broken.
- PT measures extrinsic (factor VII, warfarin); aPTT measures intrinsic (heparin, hemophilia).
- Vitamin K-dependent factors: II, VII, IX, X, C, S (mnemonic "1972 + CS").
- Anemia classification: start with MCV. <80 microcytic · 80–100 normocytic · >100 macrocytic. Then use reticulocyte count.
- Hemolysis labs: ↑ LDH, ↑ indirect bilirubin, ↓ haptoglobin, ↑ reticulocytes.
- Smear pearls: schistocytes = MAHA · spherocytes = HS/AIHA · target cells = thal/liver · sickle cells = SCD · hypersegmented neutrophils = B12/folate · Howell-Jolly = asplenia.
- Adult hematopoiesis happens in axial skeleton; extramedullary hematopoiesis (liver/spleen) appears in chronic hemolysis (β-thal major) or marrow failure.
- Febrile neutropenia (ANC <500 + fever) is a medical emergency – start broad-spectrum antibiotics immediately.
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.