Summary
Transfusion reactions are classified by onset (< 24 hours vs. > 24 hours) and mechanism. Acute immune reactions include acute hemolytic transfusion reaction (AHTR) from ABO mismatch (type II hypersensitivity; fever, flank pain, hemoglobinuria, positive Coombs; treat with aggressive IV normal saline), febrile non-hemolytic transfusion reaction (FNHTR) (most common; cytokines/anti-HLA antibodies; prevented by leukoreduction), anaphylaxis (classically IgA-deficient recipients; requires IM epinephrine and washed RBCs), and TRALI (donor anti-leukocyte antibodies causing ARDS-like noncardiogenic pulmonary edema with hypotension). Non-immune acute reactions feature TACO (volume overload with hypertension, elevated JVP/BNP, and S3; treated with IV furosemide) and citrate-induced hypocalcemia. Delayed reactions (> 24 hours) include delayed hemolytic reaction (anamnestic IgG to minor antigens like Kidd) and TA-GVHD (donor T cells attacking host marrow; prevented by irradiated blood). Emergency management mandates stopping the transfusion immediately at the first sign of a reaction.
Overview & Classification
Blood transfusion is lifesaving but carries real risks. Complications are classified along two axes: timing (acute, < 24 hours vs delayed, > 24 hours) and mechanism (immune-mediated vs non-immune). Overlaying these two axes produces the core 2×2 matrix that nearly every exam question is built on.
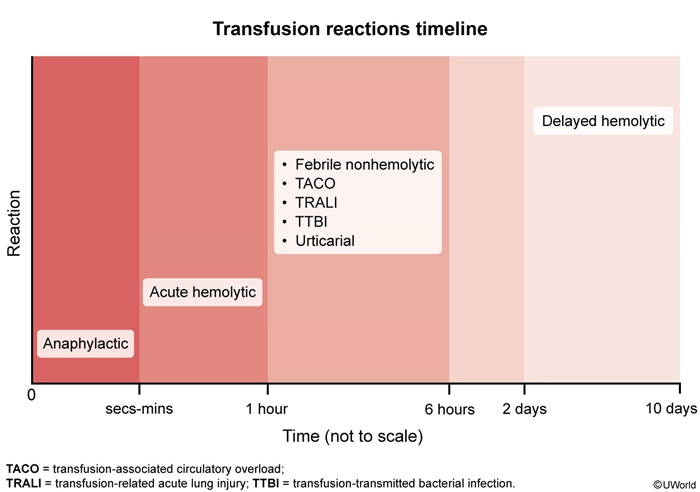
The timing of symptom onset after a transfusion is the single most useful diagnostic clue — anaphylaxis and acute hemolysis strike within seconds to minutes, febrile/respiratory reactions within 1–6 hours, and hemolytic/immunologic delayed reactions appear 2–10 days later.
| Classification of Transfusion Reactions | ||
|---|---|---|
| Timing | Immune-Mediated | Non-Immune |
| Acute (< 24 h) | AHTR (ABO mismatch); FNHTR; Allergic / Anaphylactic; TRALI | TACO; Septic (bacterial contamination); Metabolic — hypocalcemia, hyperkalemia |
| Delayed (> 24 h) | DHTR; TA-GVHD; Alloimmunization | Iron overload; Infections (HBV, HCV, HIV, CMV) |
The remainder of this lesson works through this grid: acute immune reactions, other acute reactions, then delayed complications, and finally a universal emergency protocol. The Immunologic Blood Transfusion Reactions reference organizes each immune reaction by onset, cause, and key features if you want the one-page summary.
Acute Immune Reactions (< 24 h)
Four immune-mediated reactions appear within 24 hours of transfusion. For each, anchor on mechanism, onset, key features, and the specific next step.
1. Acute Hemolytic Transfusion Reaction (AHTR)
- Mechanism: recipient preformed IgM against ABO antigens on donor RBCs → complement activation → intravascular hemolysis (type II hypersensitivity). Almost always a clerical error (wrong unit / wrong patient).
- Onset: within minutes of starting the transfusion.
- Key features: fever, chills, flank/back pain, hypotension, tachycardia, hemoglobinuria (dark urine), DIC, acute kidney injury. In an anesthetized patient, diffuse surgical-wound oozing + hypotension may be the only clue.
- Labs: ↑ LDH, ↑ indirect bilirubin, ↓ haptoglobin, positive direct Coombs (DAT), hemoglobinuria.
- Management: STOP transfusion; aggressive IV normal saline to keep urine output > 100 mL/hr; treat shock/DIC; return bag + fresh patient sample to the blood bank.
| Important – فكرة سؤال | |
|
Fever + flank/back pain + dark (hemoglobinuric) urine + hypotension within minutes of starting a transfusion = Acute Hemolytic Transfusion Reaction (ABO mismatch / clerical error). First step: STOP the transfusion, keep the line open with IV normal saline to protect the kidneys, and return the bag + a fresh patient sample to the blood bank. حمى + ألم أسفل الظهر + بول داكن + هبوط ضغط أثناء النقل ← أوقف النقل فوراً. |
تذكر |
2. Febrile Non-Hemolytic Transfusion Reaction (FNHTR)
- The most common transfusion reaction — a diagnosis of exclusion.
- Mechanism: cytokines (IL-1, IL-6, TNF) accumulated from donor WBCs during storage, or recipient anti-HLA antibodies reacting with donor leukocytes.
- Onset: 1–6 hours after the transfusion starts.
- Key features: fever (≥ 1 °C rise), chills, malaise. No hemolysis, no hypotension, no respiratory distress.
- Management: stop transfusion (must rule out AHTR), give antipyretics (acetaminophen); self-limiting. Prevent future episodes with leukoreduced products.
3. Allergic and Anaphylactic Reactions
- Mild allergic (urticarial): type I hypersensitivity to donor plasma proteins → urticaria, pruritus, flushing within minutes; no fever, no hypotension. Pause transfusion, give antihistamines (diphenhydramine); may resume slowly if symptoms resolve — the only reaction in which restarting the same unit is acceptable.
- Anaphylactic: classically an IgA-deficient recipient with anti-IgA antibodies reacting against donor plasma IgA. Onset seconds–minutes: hypotension, shock, bronchospasm/wheeze, stridor, angioedema, ± vomiting. STOP transfusion → IM epinephrine, IV fluids, airway support, antihistamines/steroids. Prevent with washed RBCs or IgA-deficient donor units.
| Note – ملاحظة | |
|
Selective IgA deficiency is the most common primary immunodeficiency. Most patients are asymptomatic but carry a lifelong risk of anaphylaxis from any blood product containing IgA. Prevent with washed RBCs or products from IgA-deficient donors. |
ملاحظة |
4. Transfusion-Related Acute Lung Injury (TRALI)
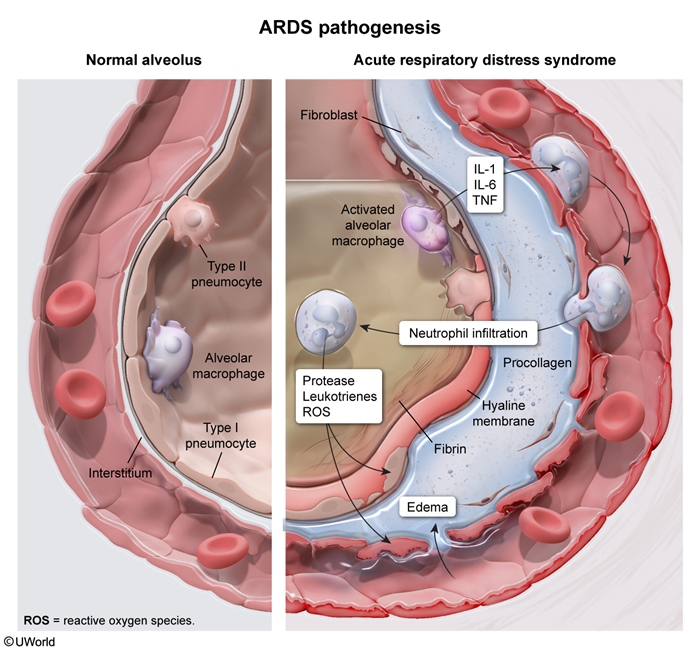
- Mechanism: donor anti-HLA / anti-neutrophil antibodies activate recipient neutrophils in the pulmonary microvasculature → capillary leak → non-cardiogenic pulmonary edema (ARDS-like).
- Onset: within 6 hours.
- Key features: acute dyspnea + hypoxia, bilateral pulmonary infiltrates, often hypotension and fever; no signs of fluid overload (normal JVP, normal BNP).
- Management: STOP transfusion; supportive oxygen / mechanical ventilation. Most recover in 24–72 h; mortality up to ~50% in previously critically ill patients. Full TRALI vs TACO comparison follows in the next section.
| Important – فكرة سؤال | |
|
TRALI is the leading cause of transfusion-related death. Dyspnea + hypoxia + bilateral infiltrates within 6 hours, often with hypotension and fever — it looks like ARDS triggered by transfusion. Treatment is supportive (oxygen, mechanical ventilation) — do NOT give diuretics (this is not volume overload). Risk factors include smoking, alcohol use, and critical illness. |
تذكر |
When fever, rash, or respiratory distress appears mid-transfusion, the differential diagnosis of acute transfusion reactions by symptom maps each cardinal symptom to its likely reaction.
Other Acute Reactions (< 24 h)
The remaining acute reactions are non-immune: circulatory overload, bacterial sepsis, and the metabolic derangements of massive transfusion.
1. Transfusion-Associated Circulatory Overload (TACO)
- Mechanism: too much volume too fast → ↑ hydrostatic pressure → cardiogenic (hydrostatic) pulmonary edema.
- Onset: during or within 6 hours of transfusion.
- Key features: dyspnea, hypertension, raised JVP, S3 gallop, peripheral edema; ↑ BNP and cardiomegaly on CXR — a classic CHF picture. Risk: elderly, CHF, renal failure, infants.
- Management: slow or stop transfusion, sit the patient upright, give oxygen and IV furosemide; transfuse slowly and in divided units in future.
Distinguishing TRALI from TACO is a perennial exam question — both cause dyspnea and bilateral infiltrates within 6 hours, but the hemodynamics and management are opposite.
| TRALI vs TACO | ||
|---|---|---|
| Feature | TRALI | TACO |
| Mechanism | Donor anti-HLA / anti-neutrophil antibodies activate recipient neutrophils → capillary leak | Volume overload → ↑ hydrostatic pressure → pulmonary edema |
| Onset | Within 6 hours | During or within 6 hours (often during transfusion) |
| Edema type | Non-cardiogenic (↑ permeability) | Cardiogenic (hydrostatic) |
| Blood pressure | Hypotension | Hypertension |
| JVP / S3 | Normal | Elevated JVP, S3, peripheral edema |
| BNP | Normal | Elevated |
| Fever | Often present | Absent |
| CXR | Bilateral infiltrates, normal heart size | Bilateral infiltrates + cardiomegaly ± effusions |
| Treatment | Stop transfusion; O₂ / supportive ventilation; do NOT diurese | Stop/slow transfusion; upright position; O₂; IV furosemide |
| Risk group | Any patient (smoking, alcohol, critical illness ↑ risk) | Elderly, CHF, renal failure, infants; fast/large volumes |
| Important – فخ امتحاني | |
|
Both TRALI and TACO cause dyspnea + bilateral infiltrates within 6 hours — blood pressure is the key separator.
فخ امتحاني: كلاهما يسبب ضيق تنفس، لكن الضغط هو الفارق الرئيسي. TRALI يسبب هبوط ضغط (Hypotension) بينما TACO يسبب ارتفاع ضغط (Hypertension). ابحث عن علامات فشل القلب في TACO. |
تذكر |
2. Septic (Bacterial Contamination) Reaction
- Mechanism: bacterial contamination of the product → endotoxin release in the recipient. Most often with platelets (stored at room temperature, ~22 °C). Organisms: Yersinia enterocolitica (cold-growing, in RBCs), Staphylococcus and gram-negatives (platelets).
- Onset: minutes to hours.
- Key features: high fever, rigors, hypotension, shock — mimics AHTR but without hemoglobinuria or back pain.
- Management: STOP transfusion → broad-spectrum IV antibiotics, IV fluids/vasopressors; culture both the patient and the bag.
Sepsis, anaphylaxis, TRALI, and AHTR all present with hypotension; the transfusion reactions associated with hypotension comparison separates the four by onset and cause.
3. Metabolic Complications of Massive Transfusion
Massive transfusion (≈ 1 blood volume / ~10 units in 24 h) produces predictable metabolic derangements:
- Hypocalcemia: citrate anticoagulant in stored blood chelates calcium → perioral tingling, tetany, prolonged QT; treat with IV calcium gluconate.
- Hyperkalemia: stored RBCs leak potassium → arrhythmia risk (especially renal failure, neonates).
- Also hypothermia (cold products — use a warmer) and dilutional coagulopathy/thrombocytopenia.
Refer to acute hypocalcemia: causes, features, and IV calcium treatment for the citrate mechanism and the Chvostek/Trousseau signs to look for.
Delayed Complications (> 24 h)
Delayed complications surface days to years after transfusion. Each has a signature vignette.
1. Delayed Hemolytic Transfusion Reaction (DHTR)
- Classic vignette: an unexplained drop in hemoglobin 2–10 days (often ~7 days) after a "successful" transfusion, with low-grade fever and mild jaundice.
- Mechanism: anamnestic response — the recipient was previously sensitized (prior transfusion or pregnancy) to a minor RBC antigen (most often Kidd/Jk; also Rh, Duffy, Kell). The antibody titer was too low to detect on crossmatch, then rises after re-exposure → IgG-mediated extravascular hemolysis (spleen) → no hemoglobinuria.
- Labs: positive direct Coombs, ↑ indirect bilirubin, ↓ haptoglobin, ↓ Hb.
- Management: usually supportive; identify the offending antibody so future units are antigen-negative.
2. Transfusion-Associated GVHD (TA-GVHD)
- Mechanism: viable donor T lymphocytes engraft and attack the recipient's tissues.
- At risk: severely immunocompromised patients (BMT recipients, hematologic malignancy, congenital immunodeficiency, fetus) and transfusion from a first-degree relative (shared HLA haplotype lets donor T cells evade recognition).
- Onset: 4–30 days post-transfusion.
- Key features: fever, skin rash, diarrhea, hepatitis, pancytopenia — the recipient marrow is attacked (unlike BMT-GVHD, where marrow is spared). Mortality > 90%.
- Prevention: irradiate blood products to inactivate donor lymphocytes.
| Note – ملاحظة سريرية | |
ملاحظة سريرية: تشعيع الدم (Irradiation) ضروري للمرضى ذوي المناعة المنخفضة وللتبرع من الأقارب من الدرجة الأولى لمنع TA-GVHD المميت. |
ملاحظة |
3. Iron Overload (Secondary Hemochromatosis)
- Classic vignette: a chronically transfused patient — β-thalassemia major, sickle cell disease, MDS.
- Each unit of RBCs contains ~250 mg iron and there is no physiologic excretory route, so iron deposits in heart (cardiomyopathy), liver (cirrhosis), pancreas (diabetes), skin (bronze), and gonads.
- Treatment: iron chelators — deferoxamine, deferasirox, deferiprone.
4. Alloimmunization & Transfusion-Transmitted Infections
Alloimmunization: repeated transfusion drives antibodies against donor RBC, HLA, or platelet antigens → future crossmatch difficulty, platelet refractoriness, and DHTR.
Infections are rare in modern screened banks but remain high-yield. Per-unit risk in developed countries (approximate): HBV ~1:1,000,000, HCV ~1:2,000,000, HIV ~1:2,000,000. CMV is the key pathogen for immunocompromised patients and neonates → use CMV-negative or leukoreduced units.
Emergency Management & Prevention
Regardless of the suspected reaction, the first response is identical — recognize, stop, support, and investigate before you treat by type.
- Step 1 — STOP the transfusion immediately at the first sign of any reaction.
- Step 2 — Maintain IV access with normal saline through a new line — keeps the vein open and supports blood pressure and renal perfusion.
- Step 3 — Reassess & verify: check vital signs; re-check the patient's identity against the unit label (clerical error is the #1 cause of AHTR).
- Step 4 — Send to the blood bank: the blood bag, the IV tubing, and a fresh patient blood + urine sample for repeat crossmatch, direct Coombs, and culture.
- Step 5 — Treat by reaction type: IM epinephrine for anaphylaxis; antipyretics for FNHTR; broad-spectrum antibiotics for sepsis; IV furosemide for TACO; supportive oxygen/ventilation for TRALI and AHTR (plus aggressive saline for AHTR).
| Mnemonic – جملة تذكرية | |
|
First response to ANY suspected reaction — "STOP":
|
جملة تذكرية |
Prevention — Modify the Product to Match the Patient
Targeted product modification is the primary tool for preventing recurrent or fatal reactions.
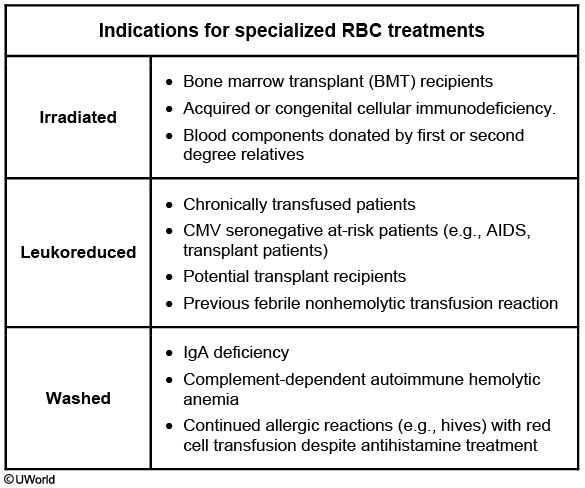
| Blood Product Modifications | ||
|---|---|---|
| Modification | Indication | Purpose / Prevents |
| Leukoreduction | Recurrent FNHTR; chronic transfusion; CMV-seronegative substitute | Removes WBCs → prevents FNHTR, HLA alloimmunization, CMV transmission |
| Irradiation | Severe immunocompromise (BMT, heme malignancy, congenital); donation from 1st-degree relative; intrauterine/neonatal | Inactivates donor T lymphocytes → prevents TA-GVHD |
| Washed RBCs | IgA deficiency with anti-IgA antibodies; recurrent severe allergic/anaphylactic reactions | Removes plasma proteins → prevents anaphylaxis |
| CMV-negative units | Pregnant women, neonates, transplant/HIV, severe immunocompromise | Avoids CMV transmission (alternative to leukoreduction) |
Prevention also starts with transfusing only when indicated — the RBC transfusion thresholds by hemoglobin level lay out the <7, 7–8, and 8–10 g/dL triggers that limit unnecessary exposure.
احصل على التجربة الكاملة
اشترك للوصول لفيديوهات الشرح التفصيلي والبطاقات التعليمية التفاعلية وأسئلة الممارسة مع تتبع التقدم.