YourMedPass
أكبر مرجع لامتحان الامتياز الأردني وامتحانات الإقامة
Multiple Endocrine Neoplasia (MEN)
Multiple endocrine neoplasia (MEN) syndromes are autosomal dominant disorders characterized by tumors in multiple endocrine glands. MEN 1 presents with the “3 P’s” – parathyroid adenomas, pituitary tumors, and pancreatic neuroendocrine tumors. MEN 2A and 2B are caused by RET proto-oncogene mutations and present with medullary thyroid carcinoma and pheochromocytoma.
The most common initial manifestation of MEN 1 is primary hyperparathyroidism (90%), while MEN 2 typically presents with medullary thyroid carcinoma. Diagnosis requires genetic testing, and management involves surveillance and surgical resection of tumors. Family members should undergo genetic screening, and prophylactic thyroidectomy is indicated for MEN 2 carriers.
Last updated: August 6, 2025
- Group of autosomal dominant inherited disorders causing tumors in two or more endocrine glands
- Three main types: MEN 1, MEN 2A, and MEN 2B
- Characterized by specific patterns of endocrine neoplasia based on genetic mutations
Multiple endocrine neoplasia type 1 (MEN1) is caused by mutations in the MEN1 tumor suppressor gene and is characterized by tumors of the Parathyroid gland, Pituitary, and Pancreas (mnemonic: the "3 Ps") ().
- Primary hyperparathyroidism
- Primary hyperparathyroidism is often the initial manifestation and usually presents with asymptomatic hypercalcemia or renal stones. Indications for parathyroidectomy in patients with MEN1, similar to those for sporadic primary hyperparathyroidism, include symptomatic hypercalcemia, end-organ complications (eg, osteoporosis, chronic kidney disease, nephrolithiasis), and an increased risk for complications (eg, urinary calcium excretion >400 mg/day). Patients age <50 are likely to develop complications later in life and should also undergo parathyroidectomy; because MEN1 typically presents at a relatively young age, most patients should be offered surgery. Patients with MEN1 usually have multiple parathyroid adenomas and therefore require subtotal (≥3½ glands) or total parathyroidectomy with autotransplant into a muscle pocket.
- Pituitary tumors
- Prolactin-secreting adenomas (prolactinomas) are the most common pituitary tumors. In premenopausal women, prolactinomas typically present with metabolic symptoms (eg, menstrual irregularities, galactorrhea); in men and postmenopausal women they usually present later when tumor enlargement leads to mass effect symptoms such as headache or bitemporal visual field deficits due to compression of the optic chiasm.
- Pancreatic tumors
- Enteropancreatic neuroendocrine tumors are the third major tumor type in MEN1. Gastrinoma (leading to Zollinger-Ellison syndrome) is the most common (eg, recurrent peptic ulcers), followed by insulinoma (eg, hypoglycemia) and nonfunctional tumors. These tumors are often metastatic and are a frequent cause of tumor-related death in MEN1. VIPomas (eg, secretory diarrhea) and glucagonoma (eg, hyperglycemia, weight loss, necrolytic migratory erythema) are other neuroendocrine tumors that can also be seen.
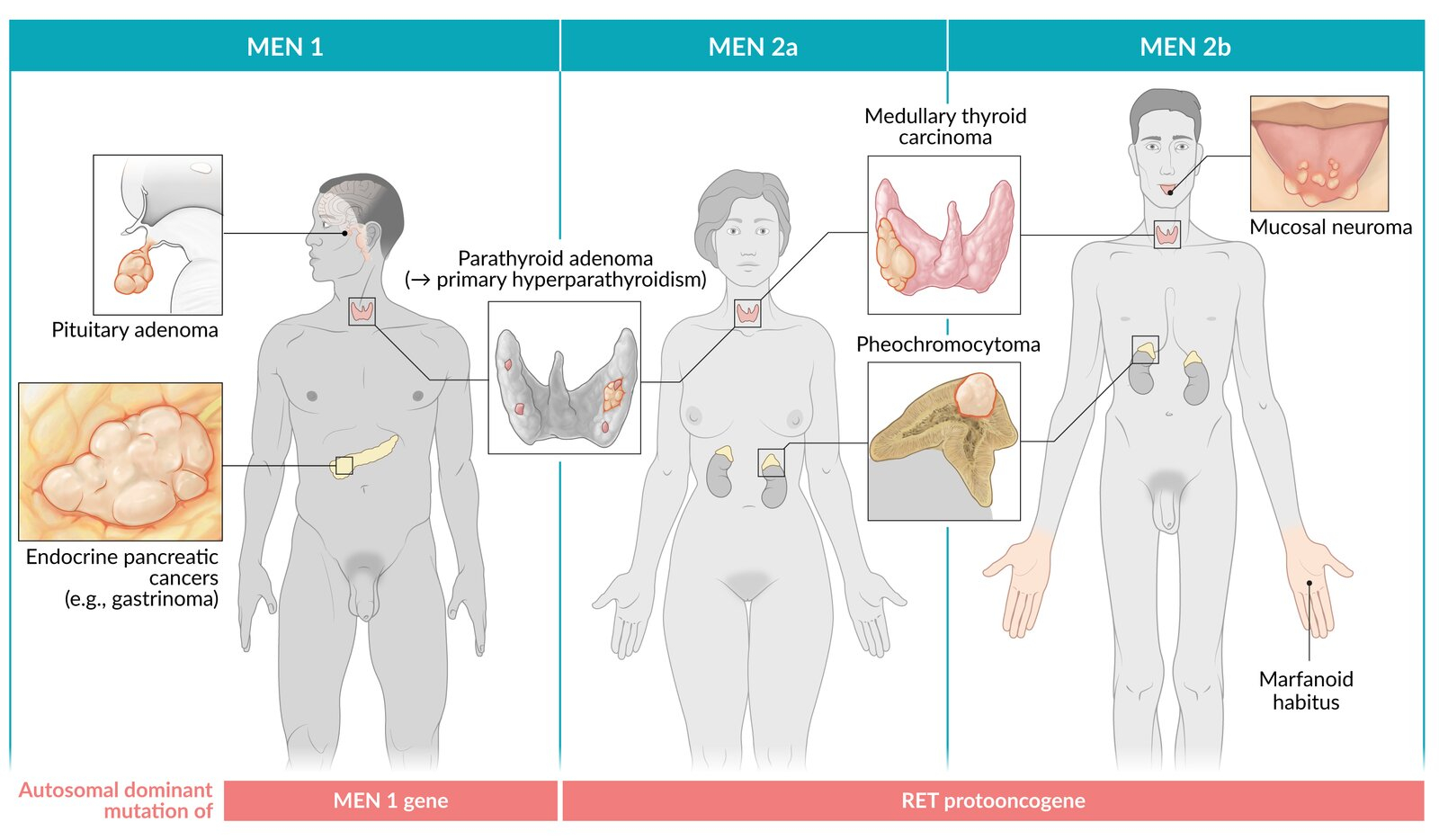
Multiple endocrine neoplasia type 2 (MEN2) is the most common inherited disorder associated with activating germline mutations of the RET protooncogene; it is characterized by the following tumors ():
- Medullary thyroid cancer
- Medullary thyroid cancer (MTC), arising from the thyroid C (parafollicular) cells, is present in nearly all patients with MEN2 and is usually more aggressive and occurs at an earlier age than sporadic MTC.
- Pheochromocytoma
- Pheochromocytoma develops in roughly half of patients with MEN2 syndromes and causes paroxysmal hypertension and tachycardia due to the intermittent secretion of catecholamines.
- Parathyroid hyperplasia or mucosal neuromas/marfanoid habitus
- Parathyroid hyperplasia (type 2A) or marfanoid habitus (eg, tall, slender build; increased limb-to-height ratio) and mucosal neuromas (type 2B) are the third characteristic seen.
Complications of MEN are related to the specific tumors and hormonal imbalances, as follows:
- Hyperparathyroidism: bone disease, kidney stones, and cardiovascular complications
- Pituitary adenomas: hormone-related complications (eg, acromegaly, Cushing disease, prolactinoma)
- Pancreatic neuroendocrine tumors: gastrointestinal symptoms, diabetes mellitus, and hormone-related syndromes (eg, Zollinger-Ellison syndrome, insulinomas)
- MTC: thyroid dysfunction, metastatic disease
- Pheochromocytoma: hypertension, cardiac arrhythmias, stroke
General Principles
- Surgical resection of tumors when indicated
- Regular surveillance for at-risk organs
- Genetic counseling for family members
MEN 1 Management
- Parathyroidectomy
- Subtotal (3.5 glands) or total with autotransplant
- Indications: symptomatic or Ca >11 mg/dL
- Pancreatic tumors
- Gastrinoma: High-dose PPI (omeprazole 60-120 mg/day)
- Surgery if >2 cm (risk of metastasis)
- Pituitary adenoma
- Prolactinoma: Cabergoline (first-line)
- Others: Transsphenoidal surgery
MEN 2 Management
Critical: ALWAYS remove pheochromocytoma BEFORE thyroidectomy to prevent hypertensive crisis
- Prophylactic thyroidectomy timing
- MEN 2B: <1 year (ideally <6 months)
- MEN 2A high-risk: <5 years
- MEN 2A lower risk: 5-10 years
- Pheochromocytoma
- Alpha-blockade first (phenoxybenzamine)
- Beta-blockade only after alpha-blockade
- Adrenalectomy after adequate blockade
Multiple endocrine neoplasia type 1 can be remembered by the "3 Ps" (Parathyroid gland, Pituitary, and Pancreas), whereas types 2A and 2B have medullary thyroid cancer and pheochromocytoma in common ().
| MEN Type Mnemonics | |
|
MEN 1 = 3 P's
MEN 2A = 2PM
MEN 2B = 2MP
|
جملة تذكرية |
| Inheritance Pattern | |
|
"MEN-tal dominance" Remember that MEN syndromes have autosomal dominant inheritance - they require MEN-tal dominance! |
جملة تذكرية |
| Classic Presentations | |
|
MEN 1: "Young patient with kidney stones and peptic ulcers" MEN 2A: "Bilateral pheochromocytomas" MEN 2B: "Teenager with bumpy tongue and marfanoid appearance" |
جملة تذكرية |